Article Text

Abstract
BACKGROUND In patients with alcoholic liver cirrhosis, endotoxaemia is a frequent finding. Unknown mechanisms, however, prevent typical clinical symptoms of endotoxaemia in many patients.
METHODS We determined plasma levels of pro- and anti-inflammatory mediators, ex vivo cytokine secretion capacity, and expression of tumour necrosis factor (TNF) receptors on phagocytic blood cells in 49 patients with alcoholic cirrhosis and 41 age matched healthy controls.
RESULTS In addition to increased levels of proinflammatory cytokines in cirrhotic patients, we observed consistent upregulation of the anti-inflammatory mediators interleukin 10 (IL-10) (plasma 15.75 (1.6) v6.6 (1.3) pg/ml (p<0.001); ex-vivo 108.4 (22.0)v 40.1 (7.4) pg/ml (p<0.05)), interleukin 1 receptor antagonist (plasma 527.1 (83) v331.4 (56) pg/ml (p<0.05); ex vivo 19.9 (3.4)v 10.2 (2.7) ng/ml (p<0.01)), and soluble TNF receptors (sTNF-R) in plasma (sTNF-RI 3157.2 (506.2)v 607.9 (300.3) pg/ml; sTNF-RII 3331.0 (506.2) v 1066.4 (225.1) pg/ml (p<0.001 for both)). Desensitisation at the target cell level was indicated by reduced expression of TNF receptor I on granulocytes (64.8 (6.5)v 40.1 (7.3)% positive cells; p<0.05) and unaltered plasma levels of soluble E-selectin.
CONCLUSION In patients with alcoholic liver cirrhosis, upregulation of the pro- and anti-inflammatory cytokine system and simultaneous desensitisation of effector cells could explain the restricted systemic inflammatory response to chronic endotoxaemia. This alteration in immune status may lead to impairment of host defences against infections which are frequent complications of alcoholic cirrhosis.
- liver cirrhosis
- lipopolysaccharide
- lipopolysaccharide desensitisation
- anti-inflammatory cytokines
- tumour necrosis factor
Abbreviations used in this paper
- IL
- interleukin
- IL-1ra
- IL-1 receptor antagonist
- LPS
- lipopolysaccharide
- TNF
- tumour necrosis factor
- sTNF-R
- soluble TNF receptor
- sE-selectin
- soluble E-selectin
- SIRS
- systemic inflammatory response syndrome
- AST
- aspartate aminotransferase
- ALT
- alanine aminotransferase
- GGT
- gamma glutamyltransferase
- PBS
- phosphate buffered saline
- IFN-γ
- interferon γ
Statistics from Altmetric.com
- liver cirrhosis
- lipopolysaccharide
- lipopolysaccharide desensitisation
- anti-inflammatory cytokines
- tumour necrosis factor
Endotoxins (lipopolysaccharide, LPS) are constituents of the cell wall of Gram negative bacteria. Under normal circumstances only trace amounts of endotoxin from intestinal microorganisms penetrate into the portal circulation1 to undergo clearance by the hepatic reticuloendothelial system.1 ,2 In liver cirrhosis, however, systemic endotoxaemia is common,3-5possibly as a consequence of both increased intestinal translocation3 ,6 and reduced hepatic clearance due to intra- and extrahepatic shunts and impaired activity of the reticuloendothelial system.2 Endotoxaemia is found more frequently in patients with alcohol induced cirrhosis than in patients with non-alcoholic cirrhosis.5 This finding was attributed to an alcohol related increase in intestinal permeability7and to bacterial overgrowth in the small intestine.8
Systemic administration of endotoxin in experimental models or healthy volunteers results in the release of proinflammatory mediators such as tumour necrosis factor α (TNF-α), interleukin (IL)-1β, IL-6, and IL-89 ,10 accompanied by systemic inflammatory reactions such as fever and leucocytosis. Higher systemic levels of endotoxin, as seen in critically ill patients with sepsis, may induce the systemic inflammatory response syndrome (SIRS). Despite elevated plasma endotoxin concentrations, systemic reactions are absent in most patients with liver cirrhosis and this phenomenon has been attributed to downregulation of secretion of proinflammatory cytokines as a result of chronic endotoxaemia.11 Several studies, however, have shown elevated plasma levels of TNF-α,12-15IL-1,13 IL-6,13 ,14 and IL-816in patients with liver cirrhosis. The mechanisms involved in this partial resistance or tolerance to endotoxin in patients with alcoholic liver disease are poorly understood.
Therefore, we undertook this study to investigate the mechanisms of endotoxin resistance in patients with alcoholic liver cirrhosis. In particular, we asked the following questions: firstly, is there evidence for desensitisation of peripheral blood leucocytes as a result of chronic endotoxaemia, despite increased plasma levels of proinflammatory cytokines? Such a phenomenon has been observed after acute LPS challenge in cancer patients and healthy volunteers.9 ,17 Secondly, is upregulation of proinflammatory cytokines counteracted by higher plasma levels and increased secretion by peripheral blood leucocytes of anti-inflammatory mediators? Thirdly, is there evidence for diminished reactivity at the level of the target cells, such as endothelial or phagocytic blood cells?
Patients and methods
PATIENTS AND CONTROLS
Overall, 49 patients with stable alcoholic liver cirrhosis and 41 healthy controls were studied in three subgroups. Plasma levels of endotoxin, and pro- and anti-inflammatory mediators were measured in 14 patients and 10 controls (group I). Cytokine release by LPS (100 ng/ml) stimulated peripheral blood cells and expression of surface TNF receptors on granulocytes were analysed in 23 patients and 19 controls (group II). Measurements of cytokine release were repeated in an additional 12 patients and 10 controls (group III) using three different LPS concentrations (100 ng/ml, and 10 and 50 pg/ml) thus approximating concentrations in the range of those occurring in peripheral blood in vivo.3 ,4 The three groups of patients were not different with regard to disease severity, age, or sex distributions, as shown in table 1.
Patient characteristics in the three groups
The diagnosis of alcoholic liver cirrhosis was made according to the following criteria: all patients had findings on ultrasound—that is, the presence of at least two findings such as nodular irregular surface or distorted vascular pattern or ascites, and/or histological examinations that are accepted as diagnostic of cirrhosis; a history or present findings of ascites or oesophageal varices were optional criteria. The alcoholic aetiology of liver disease was established when at least three of the following criteria were fulfilled: (a) a history of alcohol intake of more than 80 g/day for more than three years, (b) an aspartate aminotransferase/alanine aminotransferase (AST/ALT) ratio >1.5, (c) gamma glutamyltransferase (GGT) values >28 U/l, and (d) mean corpuscular volume >100 μl. To exclude patients with mild or more severe alcoholic hepatitis as a confounding variable, patients with a bilirubin concentration >85 mmol/l, AST >2.5 times the upper limit of normal, leucocytosis >10 GPt/l, or diagnostic lesions on biopsy were excluded.18 Liver biopsy was performed in 11 cases where the diagnosis of alcoholic cirrhosis or exclusion of alcoholic hepatitis remained uncertain.19 Furthermore, patients with clinical signs of infection or positive blood cultures were also excluded. None of the patients received antibiotics within 14 days prior to the study or on the day of the study.
METHODS
Blood sampling
Blood was drawn from the cubital vein on day 4 of hospital admission, at the earliest, using citrate containing pyrogen free syringes (Sarstedt, Nürnbrecht, Germany) for ex vivo blood cultures and flow cytometric analysis or heparinised syringes for measurement of plasma levels of immune mediators and endotoxin. Plasma was separated within 30 minutes in a refrigerated centrifuge (Megafuge 1.0, Heraeus, Berlin, Germany) at 4°C and 1000 g for five minutes and then stored at −70°C until analysis of endotoxin and cytokine concentrations.
Whole blood cultures
The capacity of peripheral blood cells to secrete pro- and anti-inflammatory cytokines was assessed by incubation of freshly collected whole blood, diluted 1:2 with RPMI 1640 medium (Biochrom KG, Berlin, Germany) containing 10 U/ml heparin in cryo tubes (Nunclon, Wiesbaden, Germany), for 24 hours at 37°C in the presence of 100 ng/ml of LPS Escherichia coli 0127-B8 (Sigma, Deisenhofen, Germany). Then, supernatants were recovered by centrifugation (600 g, two minutes) and stored at −70°C until determination of cytokine concentrations. In group III, in which LPS stimulation was performed at three concentrations (0.05, 0.1, and 100 ng/ml), the Milenia Ex vivo Whole Blood Stimulation Kit (DPC Biermann, Bad Nauheim, Germany) was used.
TNF receptors on phagocytes
Expression of both TNF receptor subtypes (I and II) on granulocytes and monocytes was investigated using the fluorescence labelled monoclonal antibodies, TNF-RI-PE (clone 2H10) and TNF-RII-PE (4D1B10, both Medac, Hamburg, Germany). Adequate isotype control was used for determining background staining. Leucocyte subpopulations and receptor expression were determined by triple fluorescence labelling and multiparameter flow cytometry using whole blood. Monoclonal antibodies recognising CD14, CD16, and CD45 (all Coulter Immunotech) were used for identifying and gating leucocyte populations.
Citrate anticoagulated whole blood was diluted 1:2 with phosphate buffered saline (PBS) and supplemented with sodium azide (0.1% w/v; Sigma) immediately after obtaining the blood sample; 50 μl of this suspension were incubated with 20 μl of the respective pre-titrated (1:10) antibodies (+ 4°C, light exclusion, 30 minutes). Thereafter, erythrocyte lysis and fixation of leucocytes were performed by FACS Lysing solution (Becton Dickinson) for seven minutes. After washing twice with PBS, 20 000 cells each were analysed using a FACScan instrument (Becton Dickinson). Antigen expression was determined on leucocyte subpopulations, defined by combined forward/side scatter and fluorescence gating using Lysis II software (Becton Dickinson).
Endotoxin assay
Plasma endotoxin was measured using the chromogenic limulus amoebocyte lysate assay (Coatest Endotoxin, Chromogenix, Sweden) with a lower limit of detection of 4 pg/ml. Possible endotoxin inhibitors were removed from plasma using a heating and dilution technique according to the manufacturer's guidelines. Plasma was diluted 1:2 with pyrogen free water, followed by heating of the mixture to 70°C for 10 minutes. Determinations were performed in duplicate and the mean value used.
Cytokine assays
In plasma, levels of total TNF-α, IL-12p40 (both Medgenix), bioactive TNF-α by high sensitivity (HS) assay, IL-6, IL-8, IL-1 receptor antagonist (IL-1ra), soluble TNF receptor I (sTNF-RI, p55) and II (sTNF-RII, p75), soluble E-selectin (sE-selectin) (all Quantikine), and IL-10 (Biosource) were performed in duplicate from stored samples from all patients and controls using commercially available ELISA kits. The TNF-α HS (Quantikine) test kit allows measurement of trimeric (bioactive) TNF-α in contrast with the Medgenix test kit which detects proteolytic split products of TNF-α (total TNF-α) also. Considering the short plasma half life of bioactive TNF-α in vivo, the TNF-α HS assay gives a measure of recently released bioactive TNF-α whereas the total TNF-α assay provides an integrated estimate of TNF-α release over the past hours.
TNF-α levels from whole blood LPS stimulated cell culture supernatants were determined using an automated analysing system (Immulite, DPC, Los Angeles, USA) whereas all other cytokines were measured using the same assays as for plasma.
STATISTICAL ANALYSIS
All results are given as mean (SEM). Differences between groups were evaluated for significance using the Mann-Whitney U test. To test for dose dependence of LPS stimulation, the Friedman test and the Wilcoxon test for paired samples were used. Correlation analysis between plasma endotoxin and pro- and anti-inflammatory cytokine levels in cirrhotic patients was performed using the two tailed Parson's correlation test. Differences in the frequency of endotoxaemia between groups were tested using the χ2 test with Yates' correction. Results were considered statistically significant at the 0.05 level.
Results
ENDOTOXIN CONCENTRATIONS IN PLASMA
The frequency of detectable endotoxaemia (>4 pg/ml) as well as peripheral venous endotoxin levels were significantly higher in cirrhotic patients (13/14, 16.3 (2.4) pg/ml) than in healthy controls in whom only one of 10 subjects had a positive test for endotoxin (5.9 pg/ml; p<0.001). Despite endotoxaemia, patients showed no clinical signs of an inflammatory reaction.
PLASMA CONCENTRATIONS OF PROINFLAMMATORY MEDIATORS
To investigate the possibility of a systemic response to endotoxaemia in vivo, we measured plasma levels of proinflammatory cytokines. In patients with cirrhosis, mean levels of total TNF-α, IL-6, and IL-8 were significantly higher than in controls, as shown in fig 1. Levels of bioactive TNF-α and IL-12p40 were increased but failed to reach statistical significance. In cirrhotic patients there was a significant correlation between TNF-α and IL-6 levels (p<0.01, r=0.57) but not between endotoxin and any proinflammatory cytokine.

Elevated plasma levels (mean (SEM)) of the proinflammatory cytokines total tumour necrosis factor α (TNF-α) and bioactive TNF-α (A), interleukin (IL)-6 (B), and IL-8 (C) in patients with alcoholic cirrhosis (AC, n=14) compared with healthy controls (HC, n=10) in group I. **p<0.01, ***p<0.001, AC v HC.
EX VIVO PRODUCTION OF PROINFLAMMATORY MEDIATORS
To address the question of possible LPS desensitisation of peripheral blood monocytes, we assessed LPS responsiveness of peripheral blood cells in the whole blood culture system. Surprisingly, TNF-α release in whole blood cultures was of the same magnitude in patients with cirrhosis and healthy controls (fig 2), irrespective of the LPS concentration used. This observation indicates that in vivo monocytic LPS desensitisation is very unlikely. Moreover, high dose endotoxin stimulation revealed even slightly enhanced TNF-α secretion in patient blood (fig 3A). Results were not different when TNF-α concentrations in supernatants were related to white blood cell count, monocyte, or granulocyte numbers, or when isolated peripheral blood mononuclear cells were used in culture (data not shown). The production of IL-12p40 in response to LPS was also elevated in the patient group but did not reach statistical significance (fig 3B).

The ex vivo total tumour necrosis factor α (TNF-α) secretion capacity of peripheral blood leucocytes from patients with alcoholic cirrhosis (AC, n=12) was not reduced compared with that of controls (HC, n=10), irrespective of the lipopolysaccharide (LPS) concentration used (group III). TNF-α concentrations (mean (SEM)) were measured in supernatants from cultures stimulated with LPS at 10 pg/ml, 50 pg/ml, and 100 ng/ml.

Tumour necrosis factor α (TNF-α) (A) and interleukin (IL)-12p40 (B) secretion capacity of peripheral blood leucocytes was not altered in patients with alcoholic cirrhosis (AC, n=23) compared with healthy controls (HC, n=19) in group II. Cytokine concentrations (mean (SEM)) were determined in supernatants from cultures after stimulation with lipopolysaccharide (100 ng/ml).
PLASMA CONCENTRATIONS OF ANTI-INFLAMMATORY MEDIATORS
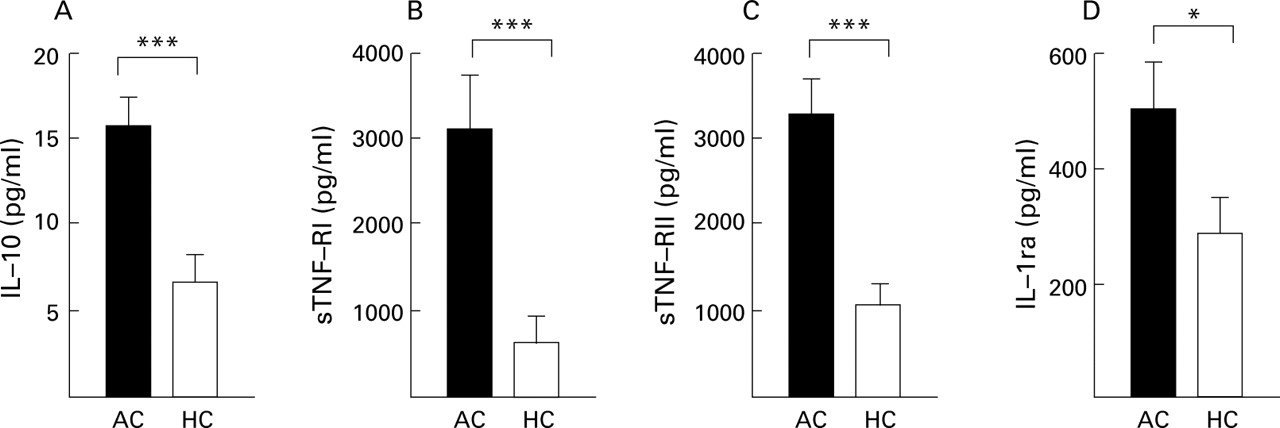
We also looked for increased levels of anti-inflammatory mediators as an indicator of counterregulation in order to balance the inflammatory potential of LPS and TNF-α. In patients, plasma concentrations of IL-10, IL-1ra, sTNF-RI, and sTNF-RII were significantly increased compared with healthy controls (fig 4). All cirrhotic patients but only 30% of controls had detectable plasma levels of IL-10 (assay sensitivity 5 pg/ml) (fig 4 A–C). In patients, there was a close correlation between plasma concentrations of both types of soluble TNF receptors (p<0.001,r=0.93) but also between total TNF-α and plasma levels of sTNF-RI (p<0.001, r=0.763) and sTNF-RII (p<0.05, r=0.61). In addition, plasma IL-10 levels were significantly correlated with IL-6 (p<0.05,r=0.62).

Elevated plasma levels (mean (SEM)) of anti-inflammatory mediators interleukin (IL)-10 (A), soluble tumour necrosis factor (TNF) receptors I (sTNF-RI) (B) and II (sTNF-RII) (C), and IL-1 receptor antagonist (IL-1ra) (D) in patients with alcoholic cirrhosis (AC, n=14) compared with healthy controls (HC, 10) in group I. *p<0.05, ***p<0.001, AC v HC.
EX VIVO PRODUCTION OF ANTI-INFLAMMATORY MEDIATORS
After LPS stimulation for 24 hours, concentrations of IL-10 and IL-1ra in supernatants from whole blood cultures were significantly higher in patients than in controls (fig 5). The ratio of TNF-α/IL-10 was not altered in cirrhotic patients because release from cultured cells of both IL-10 and TNF-α had increased. Furthermore, even spontaneous IL-1ra release without LPS stimulation was increased significantly in the patient group (fig 5B).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Interleukin (IL)-10 (A) and IL-1 receptor antagonist (IL-1ra) (B) secretion capacity of peripheral blood leucocytes was elevated in patients with alcoholic cirrhosis (AC, n=23) compared with healthy controls (HC, n=19) in group II. Cytokine concentrations were measured in supernatants of whole blood cultures after stimulation with or without lipopolysaccharide (LPS) (100 ng/ml). *p<0.05, **p<0.01, AC v HC.
TNF RECEPTOR EXPRESSION ON PHAGOCYTES
Searching for a possible source for increased plasma levels of soluble TNF receptors in cirrhotic patients, we found a significant overall reduction in TNF-RI expression on granulocytes but not on monocytes. TNF-RII expression on both granulocytes and monocytes did not differ from that in healthy controls (table 2).
Tumour necrosis factor (TNF) receptor subtype expression on granulocytes and monocytes from patients with alcoholic cirrhosis (AC, n=23) and healthy controls (HC, n=19) in group II
SOLUBLE E-SELECTIN
Finally, the question of potential activation of non-immune cells, particularly endothelial cells, was evaluated by measuring plasma sE-selectin as a marker for activation of endothelial cells. sE-selectin levels were not elevated in patients (mean (SEM): 63.2 (7.3) ng/ml, range 30–117) compared with controls (mean 40.0 (7.7) ng/ml, range 9–82; NS). There was no correlation between sE-selectin and plasma levels of either endotoxin or any other mediator.
Discussion
Despite elevated plasma levels of endotoxin, many patients with alcoholic liver cirrhosis fail to exhibit clinical signs of a systemic inflammatory reaction. The reasons for this phenomenon are unknown but may be related to induction of endotoxin tolerance in the monocyte/macrophage compartment, and/or to counterregulatory upregulation of anti-inflammatory mediators, and/or to establishment of tolerance to the action of proinflammatory mediators at the level of the distal target cells.
ABSENCE OF DESENSITISATION OF BLOOD MONOCYTES
Contrary to the hypothesis of inflammatory cell desensitisation, we found an increase in plasma levels of several proinflammatory cytokines, such as TNF-α, IL-6, and IL-8, as well as systemic endotoxaemia in patients with liver cirrhosis, thus confirming previous reports.12-16 Most likely, this finding results from endotoxin induced activation of monocytes and tissue macrophages, particularly Kupffer cells.12 ,13 Interestingly, plasma concentrations of bioactive TNF-α were not elevated to the same degree as concentrations of total TNF-α. The presence of TNF degradation products is compatible with the view that TNF-α is secreted predominantly during repetitive peaks of endotoxaemia followed by periods of TNF-α degradation by plasma proteases such as neutrophil elastase, which was found to be elevated in cirrhosis.20
In agreement with elevated plasma levels of proinflammatory mediators, our analysis of the capacity of the patients' monocytes for ex vivo LPS stimulated cytokine production revealed no impaired responsiveness compared with controls. Moreover, our findings showed a tendency for even increased secretion capacity of TNF-α and IL-12. The validity of our findings using the whole blood culture system has been corroborated by a recent report of elevated TNF-α production in isolated monocytes of cirrhotic patients.21 These observations are at variance with reports of LPS hyporesponsiveness of monocytes from cancer patients or healthy controls given a single intravenous dose of endotoxin9 ,17 or in experimental models of LPS desensitisation.22
UPREGULATION OF ANTI-INFLAMMATORY MEDIATORS
Our data provide clear evidence for upregulation of the anti-inflammatory system which may be a reaction to counteract and balance the action of proinflammatory mediators. Not only were plasma levels of IL-10, IL-1ra, sTNF-RI, and sTNF-RII elevated but in contrast with pro-inflammatory mediators, we also observed significantly higher responsiveness of patients' cells for the release of anti-inflammatory mediators such as IL-10 and IL-1ra in ex vivo whole blood cultures following LPS stimulation.
Endotoxin is capable of inducing IL-10 in monocytes and this has been shown to reduce LPS induced synthesis of TNF-α, IL-1, IL-6, IL-8, and granulocyte macrophage-colony stimulating factor (GM-CSF).23 ,24 Moreover, IL-10 downregulates granulocyte activation, interferon γ (IFN-γ) and IL-12 release, and adhesion molecule expression,25 ,26 all of which are important for an adequate host response to infection. LeMoine and colleagues21 observed diminished ex vivo IL-10 production of isolated monocytes from cirrhotic patients and suggested that this phenomenon was responsible for increased ex vivo TNF-α production by isolated monocytes. It is conceivable that these conflicting observations regarding IL-10 production may result from different culture systems. In the whole blood system a number of variables which are also present in the in vivo situation, such as plasma or granulocytes by release of prostaglandins,27 can modulate IL-10 secretion capacity.
In addition to IL-10, other anti-inflammatory mediators are upregulated in cirrhotic patients, such as IL-1ra, sTNF-RI, and sTNF-RII. IL-1ra has been found to be increased during experimental endotoxaemia28 and inhibits IL-1 action by competitive binding to the IL-1 receptor.29 When present in sufficient amounts, however, sTNF-RI and sTNF-RII exert their anti-inflammatory action by neutralising TNF-α.30
We found increased levels of soluble TNF receptors in plasma but a reduction in cell surface expression of TNF-RI on peripheral blood granulocytes but not monocytes. This pattern may well reflect granulocyte activation as shedding of TNF receptors from granulocyte membranes on activation may be one major source for soluble TNF receptors in plasma.31 Granulocytes have been shown to be a major source of IL-1ra32 and accordingly, they are the most likely source of the increased IL-1ra release in whole blood cultures in our study. Furthermore, the relative contribution to cytokine release of granulocytes may be greater than that of monocytes within the 24 hour culture period compared with more extended periods.33
DESENSITISATION OF EFFECTOR CELLS
As we could not obtain evidence for desensitisation at the level of peripheral blood monocytes, we focused on other effector cells downstream of the inflammatory cascade. Our data indicate that peripheral blood granulocytes are involved in the process of endotoxin hyporesponsiveness in cirrhotic patients. The observed loss of TNF-RI expression is compatible with a state of neutrophil exhaustion as documented in terms of impaired capacity for phagocytosis34 or production of reactive oxygen species.35 Neutrophil exhaustion may follow periods of neutrophil activation that is accompanied by increased plasma levels of neutrophil elastase.20
Furthermore, we also obtained evidence for desensitisation of a non-immune target cell population. From the observations of elevated plasma sE-selectin in systemic inflammatory response states,36 ,37 indicating an activation marker of endothelial cells, primarily one would not be surprised to find elevated levels in states of endotoxaemia also. In the present study, however, we found no elevation of sE-selectin in plasma of cirrhotic patients despite endotoxaemia and activation of inflammatory mediators. This finding supporting the idea of desensitisation of target cells is at variance with the observation of elevated plasma sE-selectin in patients with cirrhosis38 and we cannot explain this discrepancy at present. The absence of signs of endothelial cell activation may be because of the known ability of TNF-α or IL-1 to desensitise target cells for their own action,39 and therefore could indicate counterregulation at the distal target cell level. Diminished secretion of IFN-γ in cirrhotic patients40 despite slightly elevated IL-12 levels may be taken as an indicator of desensitisation of yet another target cell population, such as T lymphocytes.
In summary, in patients with repeated episodes of endotoxaemia, such as those with alcoholic liver cirrhosis, there is evidence of a chronic inflammatory response in terms of increased plasma levels of both pro- and anti-inflammatory mediators. As endotoxaemia occurs in a discontinuous fashion, it is not surprising to find no strict correlation between plasma levels of endotoxin and those of inflammatory cytokines. Analysis of peripheral blood cells for their ex vivo responsiveness to stimulation by endotoxin/LPS revealed an increased response for release of anti-inflammatory mediators while release of proinflammatory mediators was similar to that in healthy controls. This imbalance and desensitisation at the level of granulocytes or endothelial cells, as observed in the present study, may pave the way to the clinical phenomenon of endotoxin hyporesponsiveness in cirrhotic patients in vivo. Such changes in the inflammatory response to chronic endotoxaemia may also compromise host defences against infection and may be one reason for the high incidence of infectious complications and the frequent lack of typical clinical symptoms of infection in patients with liver cirrhosis. It would be interesting to test this hypothesis and investigate if interventions that reduce the rate and severity of endotoxin translocation can improve immunological function and decrease the incidence of infectious complications in patients with liver cirrhosis.
Abbreviations used in this paper
- IL
- interleukin
- IL-1ra
- IL-1 receptor antagonist
- LPS
- lipopolysaccharide
- TNF
- tumour necrosis factor
- sTNF-R
- soluble TNF receptor
- sE-selectin
- soluble E-selectin
- SIRS
- systemic inflammatory response syndrome
- AST
- aspartate aminotransferase
- ALT
- alanine aminotransferase
- GGT
- gamma glutamyltransferase
- PBS
- phosphate buffered saline
- IFN-γ
- interferon γ