Article Text

Abstract
Objective The definition of acute-on-chronic liver failure (ACLF) based on cirrhosis, irrespective of aetiology, remains controversial. This study aimed to clarify the clinicopathological characteristics of patients with hepatitis B virus-related ACLF (HBV-ACLF) in a prospective study and develop new diagnostic criteria and a prognostic score for such patients.
Design The clinical data from 1322 hospitalised patients with acute decompensation of cirrhosis or severe liver injury due to chronic hepatitis B (CHB) at 13 liver centres in China were used to develop new diagnostic and prognostic criteria.
Results Of the patients assessed using the Chronic Liver Failure Consortium criteria with the exception of cirrhosis, 391 patients with ACLF were identified: 92 with non-cirrhotic HBV-ACLF, 271 with cirrhotic HBV-ACLF and 28 with ACLF with cirrhosis caused by non-HBV aetiologies (non-HBV-ACLF). The short-term (28/90 days) mortality of the patients with HBV-ACLF were significantly higher than those of the patients with non-HBV-ACLF. Total bilirubin (TB) ≥12 mg/dL and an international normalised ratio (INR) ≥1.5 was proposed as an additional diagnostic indicator of HBV-ACLF, and 19.3% of patients with an HBV aetiology were additionally diagnosed with ACLF. The new prognostic score (0.741×INR+0.523×HBV-SOFA+0.026×age+0.003×TB) for short-term mortality was superior to five other scores based on both discovery and external validation studies.
Conclusions Regardless of the presence of cirrhosis, patients with CHB, TB ≥12 mg/dL and INR ≥1.5 should be diagnosed with ACLF. The new criteria diagnosed nearly 20% more patients with an HBV aetiology with ACLF, thus increasing their opportunity to receive timely intensive management.
- Hepatitis B
- Liver Failure
- Liver Cirrhosis
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Acute-on-chronic liver failure (ACLF) is a complex syndrome with a high short-term mortality rate.
Early diagnosis and prognosis for intensive treatment of ACLF is very important to decrease the unacceptably high mortality rate.
The definition of ACLF based on cirrhosis, irrespective of aetiology, remains controversial.
What are the new findings?
Hepatitis B virus-related ACLF exhibits clinical characteristics different from those of alcoholic liver disease-related ACLF in Western populations.
Regardless of the presence of cirrhosis, patients with chronic hepatitis B, total bilirubin ≥12 mg/dL and an international normalised ratio (INR) ≥1.5 should be included in the ACLF definition.
The new prognostic score for short-term mortality was superior to five other scores based on both discovery and external validation studies.
Nearly 20% of patients who may receive clinically intensive management were additionally diagnosed with ACLF.
How might it impact clinical practice in the foreseeable future?
The new ACLF definition bridges the gap in the European Association for the Study of the Liver-ACLF criteria for an HBV-ACLF diagnosis, and more patients may receive early and clinically intensive management, which may be useful to reduce the unacceptably high mortality.
Introduction
Acute-on-chronic liver failure (ACLF) is a complex syndrome that results in a high short-term mortality rate of 50%–90%.1–3 Recently, two large, prospective, multicentre study-based definitions, the Chronic Liver Failure (CLIF) Consortium Acute-On-Chronic Liver Failure in Cirrhosis (CANONIC)4 and the North American Consortium for the Study of End Stage Liver Diseases,5 were proposed by the European Association for the Study of the Liver (EASL) and the American Association for the Study of Liver Diseases (AASLD). These definitions describe ACLF as an acute deterioration of pre-existing chronic liver disease and define groups of patients with cirrhosis at high risk of short-term mortality. An alternative definition proposed by the Asian Pacific Association for the Study of the Liver (APASL)6 defines ACLF as jaundice (total bilirubin (TB) ≥5 mg/dL) and coagulopathy (international normalised ratio (INR) ≥1.5) complicated within 4 weeks by ascites and/or hepatic encephalopathy (HE) in a patient with or without previously diagnosed chronic liver disease. The EASL/AASLD definitions were proposed and validated only in patients with cirrhosis from Europe and North America, where alcoholic liver disease is the major aetiology; these studies included very few patients with hepatitis B virus infection, the major aetiology in the Asia-Pacific and African regions. The APASL study6 primarily enrolled patients with chronic hepatitis B (CHB) infections and lacked a specific prognostic system to assess severity. The main conflict between the EASL/AASLD and APASL definitions is what qualifies as ‘chronic’.7 HBV-related acute-on-chronic liver failure (HBV-ACLF) is a common syndrome with high mortality in the Asia-Pacific and African regions, and its clinical characteristics and progression remain unclear.8 A limited number of single-centre studies have reported a few specific epidemiological characteristics and an unacceptably high short-term mortality for HBV-ACLF,9 10 and the EASL/AASLD definitions cannot provide an accurate prognosis for these patients. This large, prospective, multicentre study clarified the distinct clinicopathological characteristics of patients with HBV-ACLF and developed evidence-based diagnostic criteria and a prognostic scoring system for patients with HBV-ACLF.
Patients and methods
Study design
Patients were prospectively screened at 13 liver centres in Chinese university hospitals and enrolled from June 2013 to October 2016. Each centre had a regular ward, an intensive treatment unit and a liver transplantation programme. The same liver transplantation allocation policy was used at all study centres.11–13 Clinical characteristics and prognostic indicators were collected to develop and validate new diagnostic criteria and a prognostic score for HBV-ACLF. Detailed clinical data and outcomes for all enrolled patients were collected and recorded in case report forms (see online supplementary materials) at admission, during hospitalisation (on days 3, 7, 14 and 21) and during the 28/90 days follow-up under the monitoring of an independent third-party company, Tigermed Consulting. The study protocol was approved by the Clinical Research Ethics Committee of the First Affiliated Hospital, Zhejiang University School of Medicine. Appropriate approvals were obtained from patients or their legal surrogates before enrolment.
Supplementary file 1
Patients
Patients who were hospitalised for at least 1 day with severe liver injury (TB ≥5 mg/dL and INR ≥1.5) from CHB10 or acute decompensation of cirrhosis (ascites/HE/upper gastrointestinal haemorrhage/bacterial infection) of all aetiologies were initially screened and enrolled in this study. The enrolment criteria for the patients with CHB corresponded to the 2009 AASLD guidelines: positive for the HBV surface antigen ≥6 months; serum HBV-DNA ≥20 000 IU/mL (105 copies/mL); persistently or intermittently elevated alanine aminotransferase/aspartate aminotransferase levels and a liver biopsy showing chronic hepatitis.14 Cirrhosis was diagnosed based on previous liver biopsy results, clinical evidence of previous decompensation and laboratory tests, endoscopy (oesophageal and gastric varices) and radiological imaging of portal hypertension and/or liver nodularity. The exclusion criteria are summarised in figure 1. During hospitalisation, all patients received integrative treatment,15–17 including a high-calorie diet; nucleoside analogues for HBV DNA-positive patients; sodium restriction, diuretics and paracentesis combined with albumin infusion for ascites; lactulose and L-ornithine aspartate for HE; prophylactic antibiotics for bacterial infections and renal replacement for hepatorenal syndrome and uremic symptoms. The detailed treatment protocol for ACLF is described in the online supplementary materials.

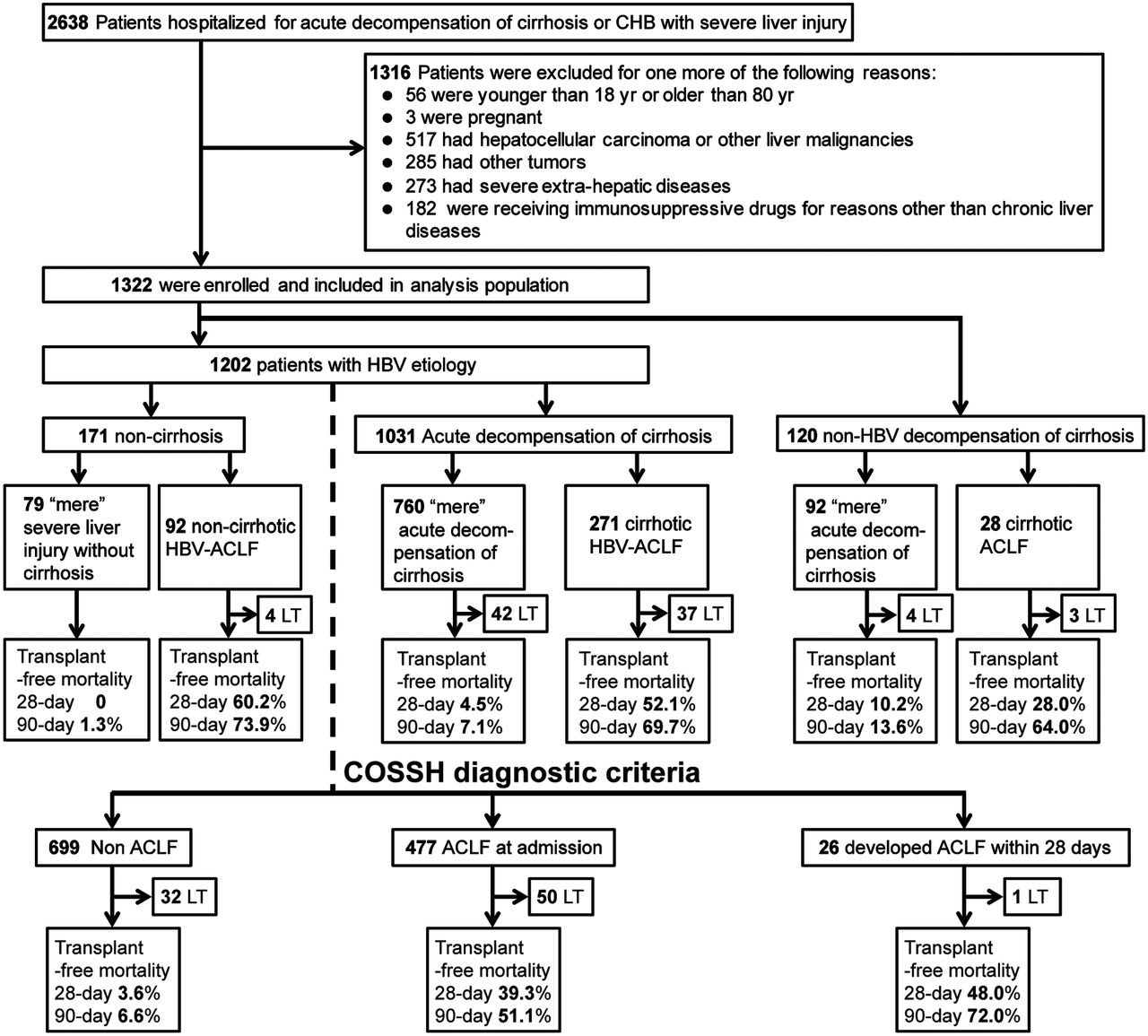
Screening, enrolment and classification of patients according to the presence or absence of EASL-ACLF or HBV-ACLF. CHB, chronic hepatitis B; COSSH, Chinese Group on the Study of Severe Hepatitis B; EASL-ACLF, European Association for the Study of the Liver-acute-on-chronic liver failure; HBV-ACLF, HBV-related ACLF; LT, liver transplantation.
Data collection
We collected the following clinical data: demographic data, admission causes, cirrhosis complications, history of episodes and precipitating events associated with acute decompensation or severe liver injury, laboratory measurements (e.g., serum albumin, sodium, alanine aminotransferase, aspartate aminotransferase, TB, INR and creatinine levels), mean arterial pressure, pulse oximetry, HBV infection biomarkers, HBV-DNA levels, antiviral treatment for HBV (nucleoside analogues, including lamivudine, adefovir, entecavir, telbivudine and tenofovir, within 6 months prior to and during hospitalisation), events of organ failure and prognosis. Survival time and information regarding liver transplantation after enrolment were also collected.
Profiling the clinical characteristics of enrolled patients
The EASL-ACLF criteria,4 with the exception of the diagnostic indicator of cirrhosis, were used to assess and identify three groups: patients with HBV-ACLF with or without cirrhosis and patients with ACLF and cirrhosis of non-HBV aetiologies (non-HBV-ACLF). The clinical and laboratory characteristics, prevalence and mortality of patients with ACLF and patients with ‘mere’ severe liver injury or decompensation were compared among the above three groups. Patients with non-cirrhotic HBV-ACLF, cirrhotic HBV-ACLF and non-HBV-ACLF were stratified into grades I, II and III using the same criteria. Short-term mortality (28/90 days) and organ failure prevalence were profiled in each group and compared with that of the patients with ACLF in the CANONIC study to determine HBV-ACLF characteristics.
Development of the HBV-ACLF diagnostic criteria
The contributions of the number and type of organ failure to 28-day mortality were analysed to develop new HBV-ACLF diagnostic criteria. Additional risk factors, such as demographic data and laboratory measurements associated with 28-day mortality, were analysed using a multivariate Cox proportional hazard (PH) model. A 28-day mortality of 15% was used as a cut-off value to define HBV-ACLF, as previously described.4 The prevalence and mortality of ACLF and the ACLF grades defined using the new diagnostic criteria were then assessed.
Development and validation of an HBV-ACLF prognostic score
Using the new HBV-ACLF diagnostic criteria, we aimed to develop a new prognostic score for patients with HBV-ACLF. Four main steps were performed. First, the Chronic Liver Failure-Sequential Organ Failure Assessment (CLIF-SOFA) score was used as a risk factor. Second, a multivariate Cox PH regression analysis including CLIF-SOFA and other clinical measurements as candidate risk factors was conducted to select the factors most associated with 28-day mortality. The prognostic model was then fitted with a multivariate linear regression analysis using the factors retained in the PH model. The coefficients estimated for each factor in the PH model that provided the best predictive ability were used as relative weights to compute the prognostic score. Third, the performance of the HBV-ACLF prognostic score was compared with the five prognostic score systems described above. Fourth, a prospective cohort of patients with HBV-ACLF admitted to the liver centre at the First Affiliated Hospital, Zhejiang University School of Medicine from January 2016 to October 2016 was created to externally validate the new model.
Statistical analysis
In univariate statistical analyses, the χ2 test was used for categorical variables and Student’s t-test and the Mann-Whitney U test were used for continuous variables. The results are presented as frequencies and percentages or means and SD. Multivariate Cox’s PH models were fitted with a forward stepwise selection method (p-in: 0.05 and p-out: 0.01) using significant baseline factors (candidate variables included TB, INR and creatinine levels and other laboratory measurements, p<0.05) that had been prefiltered in univariate PH models to identify risk factors associated with the 28-day mortality of patients with HBV aetiology or HBV-ACLF. Transplant patients were excluded from the mortality analysis.18 The prognostic model was computed using the factors retained in the PH model, with the corresponding coefficients as relative weights. The goodness-of-fit of the new prognostic score was assessed using the Hosmer-Lemeshow test. The area under the receiver operating curve (auROC) was calculated, and the Z test (Delong’s method19) was used to compare the predictive value of different prognostic scoring systems, including the Child-Turcotte-Pugh,20 Model for End-Stage Liver Disease (MELD),21 MELD-sodium (MELD-Na),22 the CLIF-Consortium Organ Failure Score (CLIF-C OFs)23 and the CLIF-Consortium-ACLF score (CLIF-C ACLFs).23 An external population of patients was enrolled to validate the performance of the prognostic score system. The scores were assessed and compared using the same methods applied to the derivation data. SPSS software V.23 (SPSS, Chicago, Illinois, USA) was used for the univariate and multivariate PH models; other analyses were conducted with R V.3.3.2 (https://www.r-project.org).
Results
Patients
A total of 1322 patients with CHB and severe liver injury (TB ≥5 mg/dL and INR ≥1.5) or with acute decompensation of cirrhosis were enrolled in this study from 2638 initially screened patients (figure 1); 1202 had an HBV aetiology with a diagnostic history of CHB (171 with non-cirrhosis, 1031 with acute decompensation of cirrhosis), and 120 had acute decompensation of cirrhosis caused by non-HBV aetiologies. Of the patients assessed using EASL-ACLF criteria4 without the diagnostic indicator of cirrhosis, 391 were diagnosed with ACLF (92 with non-cirrhotic HBV-ACLF, 271 with cirrhotic HBV-ACLF and 28 with non-HBV-ACLF), and 931 patients were diagnosed with non-ACLF (79 with ‘mere’ HBV-severe liver injury without cirrhosis, 760 with ‘mere’ HBV-acute decompensation of cirrhosis and 92 with ‘mere’ non-HBV-acute decompensation of cirrhosis). All the HBV-DNA-positive patients received antiviral therapy after hospital admission (see online supplementary table 1). Ninety patients in these groups received a liver transplant. Typical pathomorphological changes of liver cirrhosis were confirmed in 86 patients clinically diagnosed with cirrhosis in the HBV decompensation and non-HBV decompensation groups; these patients received a liver transplant. Consistent with the clinical diagnosis of non-cirrhotic HBV-ACLF, typical pathomorphological changes of liver cirrhosis were not observed in four patients who received a liver transplant (see online supplementary figure 1).
Supplementary file 2
Clinical characteristics of patients with HBV-ACLF
The clinical characteristics of all enrolled patients are summarised in table 1. Approximately 91.0% (1202/1322) of patients were diagnosed with liver diseases caused by HBV. Most patients were men. TB, INR, creatinine, serum sodium levels and white blood cell counts were significantly worse in the ACLF groups than in the non-ACLF groups. The patients with HBV-ACLF were significantly younger than those with non-HBV-ACLF. Hepatitis B relapse was the most frequent potential precipitating event in the HBV-ACLF groups (see online supplementary table 2). HBV-DNA levels in the patients with non-cirrhotic HBV-ACLF (78.3%) and cirrhotic HBV-ACLF (77.1%) were not significantly different. Liver failure was the most frequent type of organ failure observed (non-cirrhotic HBV-ACLF, 100%; cirrhotic HBV-ACLF, 93.7% and non-HBV-ACLF, 78.6%) and was significantly more frequent in the two HBV-ACLF groups (p<0.05, table 1 and online supplementary table 3). Coagulation failure was much more frequently observed in the HBV-ACLF groups than in the non-HBV group (75.0%/68.3% vs 17.9%), whereas kidney failure was more common in the non-HBV group (8.7%/14.0% vs 32.1%). Cerebral failure was more common in the non-cirrhotic HBV-ACLF group than in the cirrhotic HBV-ACLF and non-HBV-ACLF groups (17.4% vs 4.1%/7.1%). The 28-day mortality of the patients with non-cirrhotic HBV-ACLF (60.2%) and cirrhotic HBV-ACLF (52.1%) was significantly higher than that of the patients with non-HBV-ACLF (28.0%, p<0.05 for both groups).
Clinical characteristics of patients with ACLF at admission or who developed ACLF during hospitalisation
The mortality and organ failure distribution of patients with HBV-ACLF were further analysed and compared with that of the CANONIC study4 (table 2). The short-term mortality (28/90 days) rates were significantly higher in the non-cirrhotic HBV-ACLF and cirrhotic HBV-ACLF groups than in the CANONIC group (60.2% vs 32.8%, 52.1% vs 32.8%, p<0.001; 73.9% vs 51.2%, 69.7% vs 51.2%, p<0.001, respectively). A total of 63.0% (58/92) and 66.4% (180/271) of patients in the non-cirrhotic HBV-ACLF and cirrhotic HBV-ACLF groups were classified as ACLF grade 2 according to the EASL-ACLF criteria, whereas only 16.3% (15/92) and 24.4% (66/271) were classified as ACLF grade 1. The 28-day mortality rates of patients classified as ACLF grade 2 in the non-cirrhotic HBV-ACLF (58.9%) and cirrhotic HBV-ACLF (53.9%) groups were significantly higher than the rates in the CANONIC study (32.0%, p<0.001). Compared with the CANONIC study results, the prevalence of liver and coagulation failure was significantly higher and the prevalence of kidney and circulation failure was significantly lower in the HBV-ACLF groups. The prevalence of cerebral failure in patients with non-cirrhotic HBV-ACLF was lower than that reported in the CANONIC study (17.4% vs 24.1%). The prevalence of cerebral failure in patients with non-cirrhotic HBV-ACLF was significantly higher than the prevalence in patients with cirrhotic HBV-ACLF (17.4% vs 4.1%, p<0.001). The distributions of ACLF grades and organ failure in the non-HBV-ACLF group in this study were similar to those in the CANONIC study (see online supplementary table 4). The abnormal distribution among the three grades highlights the limits of the EASL-ACLF criteria for diagnosing patients with HBV-ACLF.
Short-term (28/90 days) mortality and prevalence of organ failure in patients with HBV-ACLF or with ACLF complicated by cirrhosis due to non-HBV aetiologies in the CANONIC study
HBV-ACLF diagnostic criteria
Among 1202 patients with an HBV aetiology at enrolment, 83 received liver transplants, and the remaining 1119 were examined to develop new HBV-ACLF criteria (table 3). The 28-day mortality was 21.4% for patients with failure of one organ, 61.2% in patients with failure of two organs and 96.0% in patients with failure of three or more organs. The 28-day mortality rates for patients with failure of a single organ (liver, coagulation or kidney) were higher than the predefined threshold of 15% (22.5%, 15.2% and 25.0%, respectively).
Twenty-eight-day mortality according to the number and type of organ failure and the INR or the presence of kidney dysfunction or HE grade I or II in patients with HBV aetiology at enrolment
As described in the CANONIC study,4 patients with single kidney failure were classified as having ACLF, whereas patients with single liver or coagulation failure were only included when criteria for kidney dysfunction (creatinine levels: 1.5–1.9 mg/dL) or HE grade I or II were met. In this study, 33 patients with single coagulation failure were separated into two subgroups (with and without ACLF; 28 day mortality: 25.0% and 13.8%, respectively). However, 84.4% (233/276) of patients with single liver failure did not have kidney dysfunction and/or HE grade I or II; this group exhibited a high 28-day mortality of 20.2% and did not meet the EASL-ACLF criteria.
Among these 233 patients, some progressed and died quickly, whereas others were more stable and survived. Furthermore, the multivariate Cox PH analysis indicated that the INR was the most important risk factor associated with 28-day mortality (HR 5.440; 95% CI 1.525 to 19.403; see online supplementary table 5-6). The re-estimation analysis revealed 28-day mortality rates for patients with a TB ≥12 mg/dL and an INR <1.5, 1.5≤INR<2.0 and 2.0≤INR<2.5 of 6.7%, 15.3% and 29.9%, respectively (table 3), indicating that the INR is an important indicator that may identify patients with an HBV aetiology who have a higher mortality risk.
Based on these results, patients with an HBV aetiology, single liver failure (TB ≥12 mg/dL) and an INR ≥1.5 should be diagnosed with ACLF, regardless of the presence of cirrhosis. Our new definition identified HBV-ACLF (Chinese Group on the Study of Severe Hepatitis B-ACLF, COSSH-ACLF) as a complicated syndrome with a high short-term mortality rate that develops in patients with HBV-related chronic liver disease regardless of the presence of cirrhosis and is characterised by acute deterioration of liver function and hepatic and/or extrahepatic organ failure. The new diagnostic criteria were used to classify the following three groups:
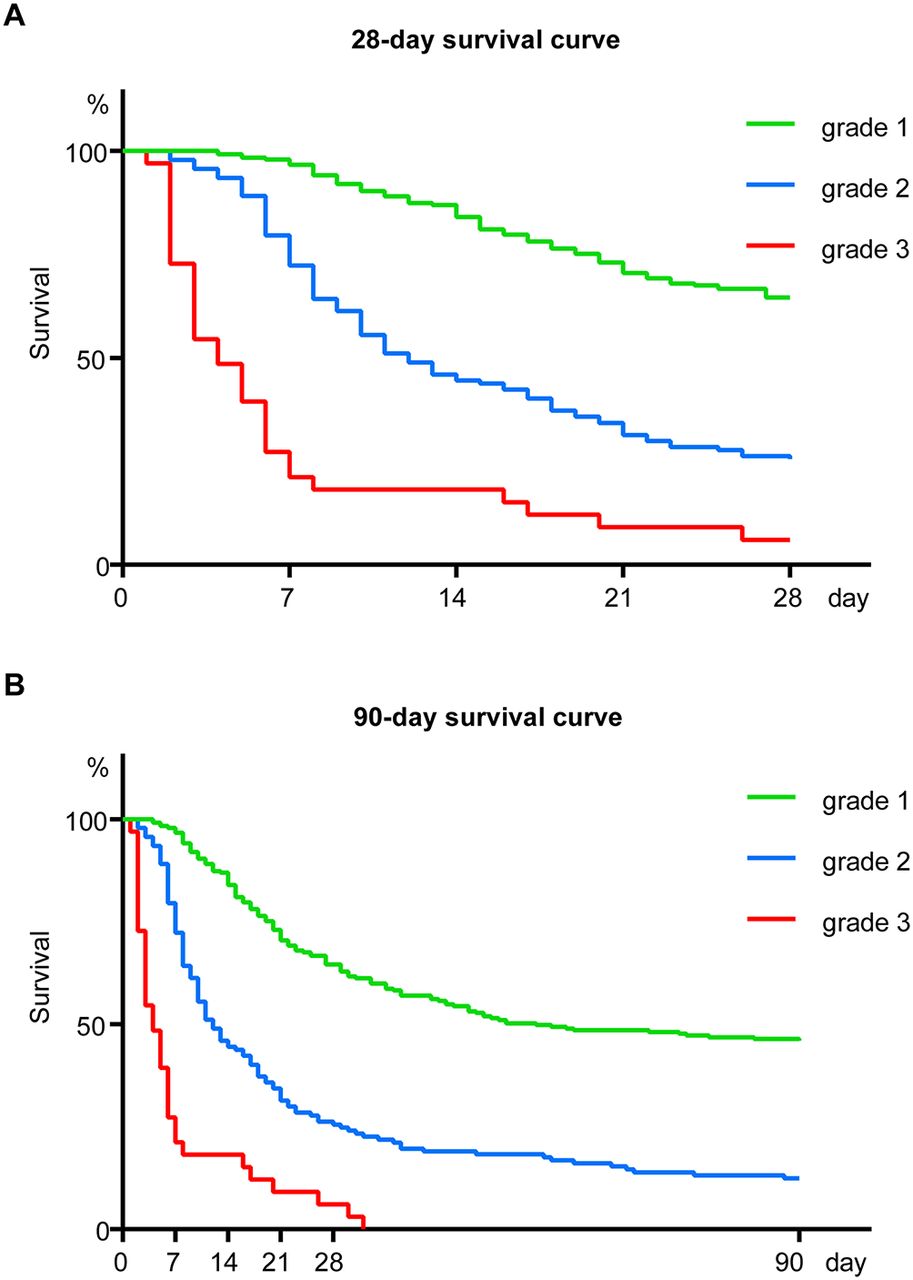
ACLF grade 1. This group includes four subgroups: (1) patients with kidney failure alone; (2) patients with single liver failure with an INR ≥1.5 and/or kidney dysfunction and/or HE grade I or II; (3) patients with single type of organ failure of the coagulation, circulatory or respiratory systems and/or kidney dysfunction and/or HE grade I or II and (4) patients with cerebral failure alone plus kidney dysfunction. Three hundred and five patients were classified as ACLF grade 1. The 28-day and 90-day mortality rates were 23.2% and 35.9%, respectively.
ACLF grade 2. This group includes patients with failures of two organ systems; 166 patients were classified as ACLF grade 2. The 28-day and 90-day mortality rates were 60.5% and 73.5%, respectively.
ACLF grade 3. This group includes patients with failures of 3 or more organ systems; 32 patients were classified as ACLF grade 3. The 28-day and 90-day mortality rates were 93.1% and 100%, respectively.
Based on the COSSH-ACLF criteria, 41.8% (503/1202) of the enrolled patients with an HBV aetiology were diagnosed with ACLF (477 were diagnosed with ACLF at admission; 26 patients were diagnosed with ACLF within 28 days after admission), whereas only 22.5% (271/1202) were diagnosed with ACLF using the EASL-ACLF criteria (figure 1, bottom and table 4). A total of 19.3% ((503−271)/1202) more patients were diagnosed with ACLF using the new diagnostic system. Approximately 94.8% (477/503) of patients were diagnosed with ACLF at admission, whereas only 58.3% (158/271) were simultaneously diagnosed using the EASL-ACLF criteria (table 4, see online supplementary table 5-6), indicating that the COSSH-ACLF criteria were significantly more sensitive than the EASL-ACLF criteria for diagnosing patients with HBV-ACLF (94.8% vs 58.3%, p<0.001). Approximately 60.6%, 33.0% and 6.4% of patients were classified as ACLF grades 1, 2 and 3, respectively, whereas 24.7%, 65.7% and 9.6% of 271 patients were classified as ACLF grades 1, 2 and 3, respectively, using the EASL-ACLF criteria, indicating that the COSSH-ACLF criteria generated a much more reasonable distribution of disease severity. The short-term mortality rates (28/90 days) of patients with newly diagnosed ACLF grade 1 disease were lower than those of patients with cirrhotic HBV-ACLF grade 1, indicating that the COSSH-ACLF criteria were better able to provide a timely diagnosis (table 4 and figure 2).
Number of patients with different ACLF grades and short-term (28/90 days) mortality of patients with HBV-ACLF under COSSH and EASL criteria

The survival curve of patients with HBV-related acute-on-chronic liver failure (HBV-ACLF) diagnosed using Chinese Group on the Study of Severe Hepatitis B-ACLF criteria. (A) 28-day survival curve of patients with HBV-ACLF. (B) 90-day survival curve of patients with HBV-ACLF.
Development and validation of a prognostic score for HBV-ACLF
The systemic analysis indicated that organ failure, an important risk factor assessed in CLIF-SOFA, was significantly associated with the 28-day mortality of patients with HBV-ACLF. A multivariate Cox PH analysis including CLIF-SOFA and other clinical and laboratory indicators was used to select the most significant combination of factors and to design an accurate prognostic score for patients with HBV-ACLF (see online supplementary table 8-9). The combination of INR, CLIF-SOFA, age and TB levels yielded the best performance, implying that TB levels and INR have clinical prognostic value in patients with HBV-ACLF. Therefore, we proposed a new HBV-SOFA (see online supplementary table 10), which represented a simplified CLIF-SOFA excluding the TB levels and INR and fit the multivariate Cox PH model again (see online supplementary table 11). Using the factors included in the PH model and corresponding coefficients, the prognostic score for patients with HBV-ACLF (COSSH-ACLFs) was calculated using the following formula: COSSH-ACLFs=0.741×INR+0.523×HBV-SOFA+0.026×age+0.003×TB level. Compared with five generic prognostic scoring systems, the COSSH-ACLFs yielded a significantly more accurate prognosis, with the highest auROC for predicting the 28/90 days mortality of patients with HBV-ACLF (28/90 days mortality: 0.829 and 0.828, table 5 and figure 3) and non-HBV-ACLF (28/90 days mortality: 0.953 and 0.793, see online supplementary table 12). An analysis of an external validation group of 154 patients (table 5) confirmed a similar predictive value of COSSH-ACLFs (28/90 days mortality: 0.813 and 0.808, table 6). The subsequent follow-up showed that the 71 patients additionally diagnosed with HBV-ACLF in the external validation group had a significantly lower 28-day morality compared with the 232 patients additionally diagnosed with HBV-ACLF in the derivation group (12.7% vs 25.0%, p<0.05, see online supplementary table 13).
Characteristics of patients with HBV-ACLF included in the derivation and validation groups

{kind=link}
{kind=link}
{kind=link}
Receiver operating curves (ROC) for the abilities of prognostic models to predict the 28-day and 90-day mortality of patients with HBV-ACLF. (A–B) ROC curves for the abilities of the prognostic models to predict the 28-day (A) and 90-day (B) mortality of the HBV-ACLF derivation group. (C–D) ROC curves for the abilities of the prognostic models to predict the 28-day (C) and 90-day (D) mortality of the HBV-ACLF validation group. ACLF, acute-on-chronic liver failure; CLIF-C OFs, CLIF-Consortium Organ Failure Score; COSSH-ACLF, Chinese Group on the Study of Severe Hepatitis B-ACLF; CTP, Child-Turcotte-Pugh; HBV-ACLF, HBV-related ACLF; MELD, Model for End-Stage Liver Disease; MELD-Na, MELD-sodium.
Comparison of the predictive value of prognostic scoring systems for patients with HBV-ACLF
Discussion
Researchers have recognised that definitions of chronic liver diseases should include cirrhosis and non-cirrhosis.7 In this prospective study based on the enrolment standards of the APASL consortium and the EASL definition of ACLF, most patients had HBV-related chronic liver disease (91%), and 171 did not have cirrhosis. When the EASL-ACLF criteria without cirrhosis were used, 92 additional patients with an HBV aetiology without cirrhosis were diagnosed with ACLF. Based on the pathology analysis, clinically diagnosed HBV-ACLF was observed in populations without cirrhosis. Liver and coagulation failures were the most common types of organ failure in patients with HBV-ACLF,9 10 whereas kidney and cerebral failure were more frequently observed in patients with non-HBV-ACLF.4 5 The short-term (28/90 days) mortality of patients with HBV-ACLF was significantly higher than that of patients with non-HBV-ACLF. As we and others have reported, hepatitis B relapse, superimposed infections with other hepatitis viruses (A or E) and mutations resistant to antiviral treatment are frequent precipitating events that may be related to the high mortality in patients with HBV-ACLF.24–26 Other potential factors, such as biochemistry, physiology and systemic inflammatory response syndrome, also need further clarification.27 These results demonstrate that patients with HBV-ACLF have specific clinical characteristics (higher severity and mortality, higher prevalence of liver failure, lower prevalence of renal failure and precipitating events) that differ markedly from those of the patients with alcohol-related ACLF in the EASL and AASLD studies, indicating that the different phenotypes are due to different aetiologies. Patients with high short-term mortality in non-cirrhotic HBV populations should be diagnosed with ACLF.
The above clinical characteristics indicate the need for an appropriate alternative definition of HBV-ACLF that is clinically helpful for early diagnosis, management and prognosis. The EASL/AASLD-ACLF criteria were appropriate for diagnosing patients with cirrhosis with both alcoholic and HBV aetiologies.9 10 28 However, they are less sensitive for the early diagnosis of patients with ACLF and an HBV aetiology. As Shi et al showed, populations with an HBV aetiology in which ACLF was precipitated by both hepatic and extrahepatic insults had significantly higher short-term mortality (28-day mortality: 48.3% and 50.7%, respectively).10 In our study, ACLF grades 2 and 3 (particularly grade 2) were more frequently observed in patients with HBV-ACLF, indicating that early identification of ACLF may not be possible with the EASL-ACLF criteria. Our results also revealed a similarly high short-term mortality in patients with both cirrhotic HBV-ACLF (28/90 days mortality: 52.1%/69.7%) and non-cirrhotic HBV-ACLF (28/90 days mortality: 60.2%/73.9%). Nearly 85% (233/276) of patients with single liver failure without kidney dysfunction and/or HE exhibited a 20.2% 28-day mortality and were not diagnosed with ACLF using the EASL-ACLF criteria. This high short-term mortality rate exceeds the predefined mortality rate of 15% and would not provide sufficient time for intensive treatments. Therefore, more sensitive diagnostic criteria for HBV-ACLF are urgently needed. Limited retrospective studies and APASL consortia indicate that liver and coagulation failures are the most frequent types of organ failure that initially result in ACLF in patients with an HBV aetiology.6 9 10 Moreover, the presence of liver and coagulation failures was significantly higher in populations with HBV-ACLF than in the populations in the CANONIC study. The 28-day mortality of patients with a TB ≥12 mg/dL and an INR ≥1.5 was 15.3%, suggesting that the INR is an important indicator for identifying the patients with HBV-related chronic liver disease that have a higher risk of mortality. Based on the EASL-ACLF criteria, our new definition of HBV-ACLF (COSSH-ACLF) ignored cirrhosis as a diagnostic indicator and yielded a more reasonable distribution (ACLF grades 1–3: 60.6%, 33.0% and 6.4%, respectively) and a higher predictive value for disease severity (28/90 days mortality of patients with ACLF grades 1–3: 23%/36%, 61%/74% and 96%/100%, respectively). Compared with the EASL-ACLF criteria, our criteria diagnosed an additional 19% of patients with ACLF and identified an additional 36% on admission; this earlier diagnosis of ACLF may allow these additional patients to receive timely clinically intensive management.
A recently developed simplified organ function scoring system (CLIF-C OFs) and a specific prognostic score for ACLF (CLIF-C ACLFs) is superior to the MELD and MELD-Na scores for predicting mortality23 in patients with ACLF with an alcoholic and cirrhotic aetiology. This study also aimed to develop an appropriate prognostic score for HBV-ACLF (COSSH-ACLFs) based on the new criteria. Our comparative analysis showed that the new COSSH-ACLFs, which includes the INR and TB levels, had the highest prognostic value for predicting the 28/90 days mortalities of patients with HBV-ACLF among the five generic scoring systems. An external prospective cohort further validated the prognostic accuracy of this system for patients with HBV-ACLF. The follow-up analysis indicated that the additional patients diagnosed with HBV-ACLF using the new criteria had a significantly lower 28-day mortality. This decrease may be associated with more patients receiving early and intensive management.29 Thus, our new COSSH-ACLFs, which was derived from an HBV-ACLF clinical database that includes the most common clinical management indicators, shows great prognostic accuracy and may be used to predict severity in patients with HBV-ACLF.
In summary, HBV-ACLF exhibits clinical characteristics that differ from those of alcoholic liver disease-related ACLF in Western populations. Regardless of the presence of cirrhosis, HBV-infected patients with chronic liver disease and a TB ≥12 mg/dL and an INR ≥1.5 have a higher short-term mortality, which should be included in the ACLF definition. Our newly proposed COSSH-ACLF bridges a gap in the EASL-ACLF criteria for an HBV-ACLF diagnosis; compared with the EASL-ACLF, the COSSH-ACLF identified approximately 20% more patients with ACLF who can receive earlier clinically intensive management. The COSSH-ACLFs provides an accurate prognosis and may help predict the severity of patients with HBV-ACLF; however, it requires further validation with dynamic observables.
Acknowledgments
The authors thank Dr Vicente Arroyo (Liver Unit, Hospital Clinic, University of Barcelona) for giving helpful comments in data analysis
and Dr Xin Chen (Institute of Biochemistry, College of Pharmaceutical Sciences, Zhejiang University) for critical review and confirmation of statistical methods and results.
References
Footnotes
TW, JL and LS contributed equally.
Contributors TW, JL and LS contributed equally. The study was designed by JL and supervised by JL and LL. The manuscript was written by JL, TW, JL and LS. The experiment and data analysis were performed by JL, TW, JL, LS, JX, LJ, QZ, DS, JJ, SS, LJ, PY, LY, YL, TL, JH, XX, JC, SH, YC, SX, ZG, ZD, TH, YW, JG, TF, CP, YC, HL, YH, QX and SL. All authors were involved in critical revision of manuscript.
Funding This work was supported by National S&T Major Project of China (2012ZX10002004-001, 2017ZX10304402-002-002), National Natural Science Foundation of China (81571818/81771996) and Zhejiang Provincial and State’s Key Project of Research and Development Plan of China (2016YFC1101303/4, 2016C01G2010737).
Competing interests None declared.
Patient consent Obtained.
Ethics approval Clinical Research Ethics Committee of the First Affiliated Hospital, Zhejiang University School of Medicine.
Provenance and peer review Not commissioned; externally peer reviewed.