



Article Figures & Data
Figures
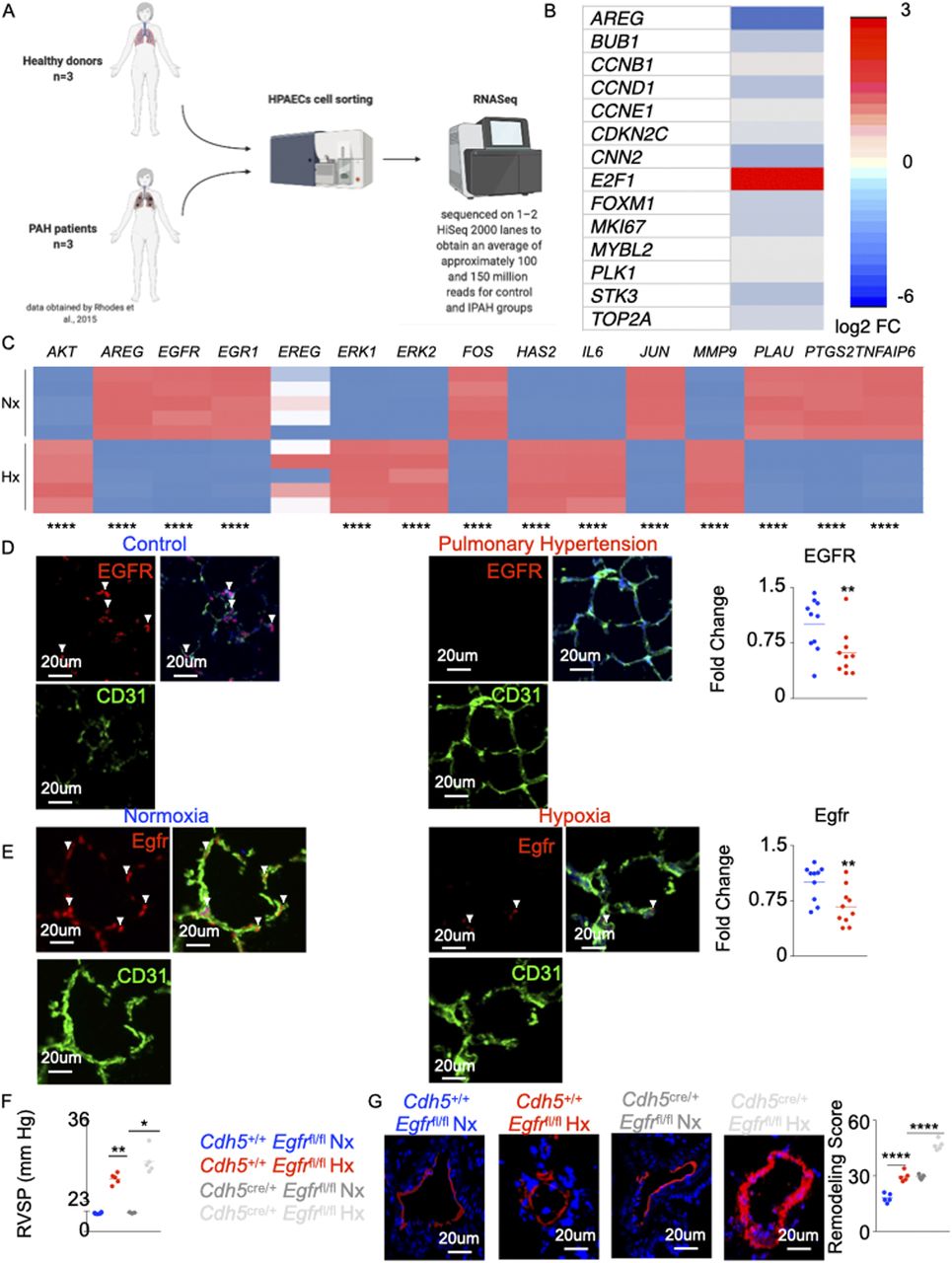
- Figure 1. Deficiency in AREG/Egfr aggravates pulmonary hypertension.
RNA sequencing data (dbGaP genotype files: phs000998.v1.p1 NHLBI/iPSC_PulmonaryHypertension) (Rhodes et al, 2015) were analyzed. Lungs of pulmonary arterial hypertension patients and healthy controls were collected (n = 7 for controls and 6 for pulmonary arterial hypertension patients). Lungs of hypoxic and normoxic mice were harvested (n = 5 for each group). (A) The flowchart depicts the analysis of the RNASeq data obtained by Rhodes et al (2015). (B) Heat map depicting expression of the cell survival genes (expressed as log2 FC) obtained from the RNASeq analysis. (C) Heat map showing expression of the genes downstream to AREG using qRT-PCR in human pulmonary endothelial cell line. (D, E) Confocal imaging of human (D) and mouse (E) lungs showing expression of EGFR (green) in CD31 (white)-expressing endothelial cells. Smooth muscle actin (SMA) (red) was used to stain the medial layer. The arrows depict EGFR+ vascular endothelial cells. (F, G) In normoxic and hypoxic Cdh5cre/+ Egfrfl/fl and littermate control mice, right ventricular systolic pressure (F) and lung vasculature remodeling (G) were quantified. n = 5 per group. Data are shown as mean. *P < 0.05, **P < 0.01, ****P < 0.001.
- Figure S1. Egfr expression is decreased in mouse and rat models of pulmonary hypertension.
(A) Schematic representing genes downstream to AREG determined using the Ingenuity Pathway Analysis Software. The solid and dotted arrows represent either direct or indirect activations, respectively. (B, C) AREG expression was evaluated in pulmonary ECs of hypoxic mice (B) and pulmonary hypertension patients (C) by confocal imaging. (D, E) Egfr-expressing ECs and Egfr MFI were assessed in lung ECs of Il6tg mice housed in hypoxic conditions (D) and monocrotaline-injected rats (E) by confocal microscopy. n = 10 replicates per condition. Data are shown as mean. **P < 0.01, ***P < 0.001, ****P < 0.0001.
- Figure S2. The levels of pulmonary endothelial Egfr, caspase 3, and Bad are altered across 3 rodent models of pulmonary hypertension.
(A, B) Wild-type and Il6tg mice were exposed to hypoxia for 3 wk. Rats were injected with either monocrotaline or vehicle diluent. (A, B) The levels of pulmonary endothelial Egfr, caspase 3, (A) and Bad (B) were assessed by confocal imaging. (C) Representative hemodynamics traces of hypoxic Cdh5Cre/+ Egfrfl/fl and Cdh5+/+ Egfrfl/fl mice. (D) Ki-67–expressing ECs and Ki-67 MFI were assessed in lung ECs of the control and Egfr KO mice. n = 5 replicates per condition. Data are shown as mean. *P < 0.05, ***P < 0.005, ****P < 0.001.
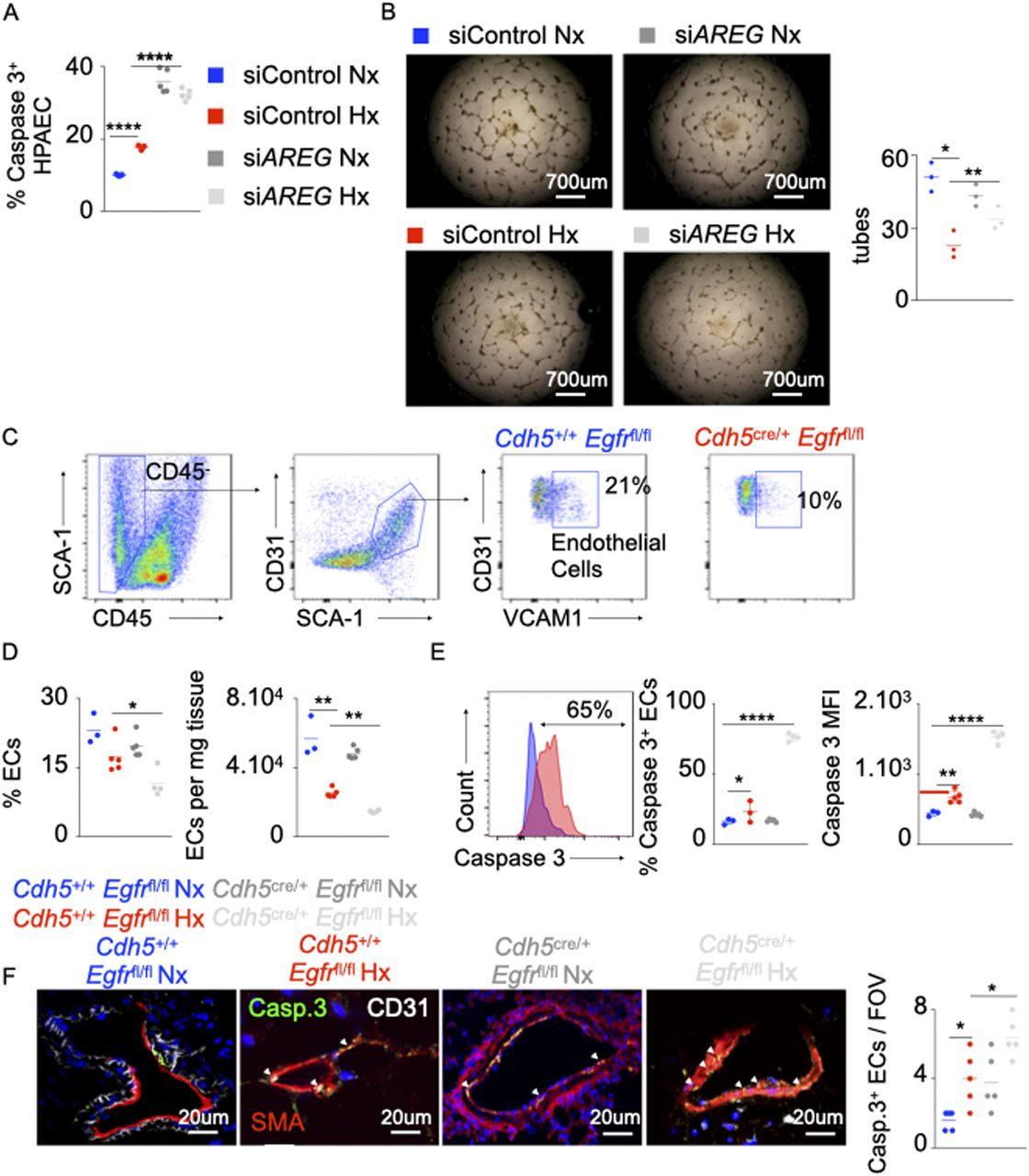
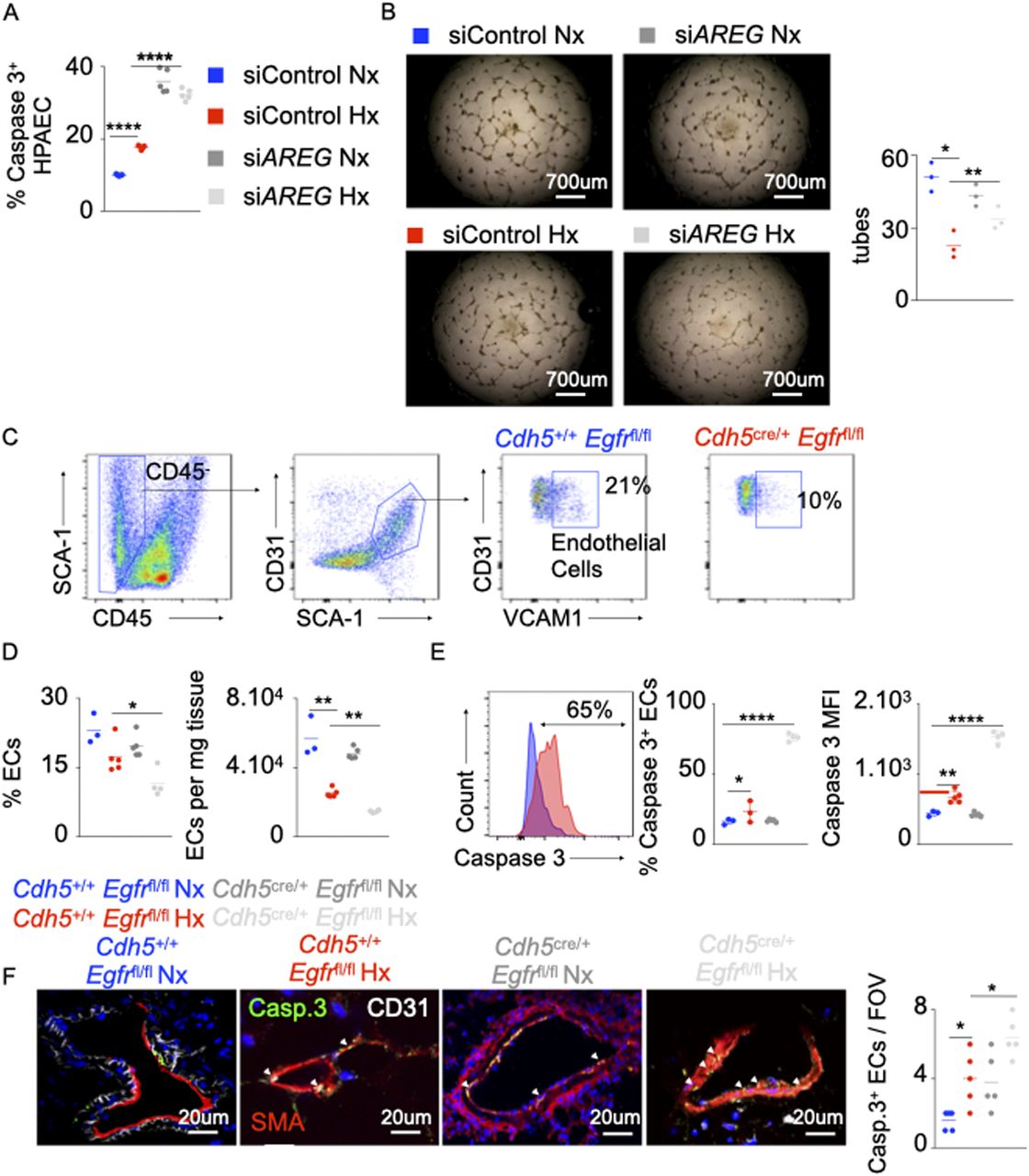
- Figure 2. The loss of AREG and Amphiregulin receptor epidermal growth factor receptor (EGFR) increases EC apoptosis.
(A, B) Pulmonary arterial endothelial cells were transfected with either scrambled siRNA (siCTL) or siRNA against AREG (siAREG) and placed in hypoxia or normoxia. (A) The cells were stained for caspase 3, and apoptosis was measured by flow cytometry. (B) Pulmonary arterial endothelial cells were plated on Matrigel, and tubular structures were photographed 4–6 h after plating. The number of tubes was quantified. (C, E) Cdh5+/+ Egfrfl/fl and Cdh5cre/+ Egfrfl/fl mice were placed in normoxia or hypoxia for 21 d, and lung vascular endothelial cells were analyzed by flow cytometry. (C, D) Flow cytometric quantification of lung vasculature endothelial cells. (E, F) The percentage of apoptotic lung vascular endothelial cells was assessed using caspase 3 staining by flow cytometry (E) and confocal microscopy (F). n = 5 per condition. Data are shown as mean. *P < 0.05, **P < 0.01, ****P < 0.001.
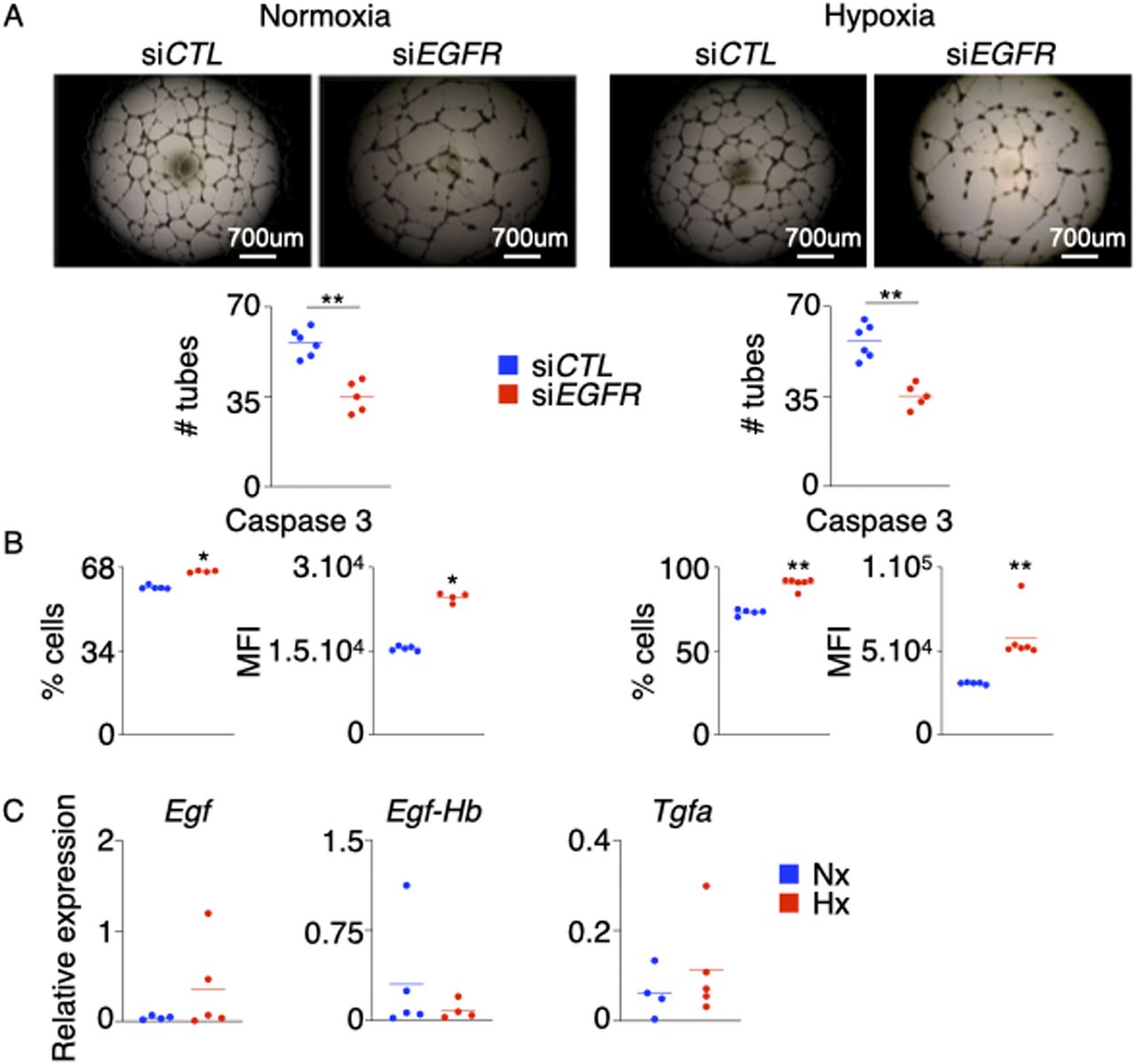
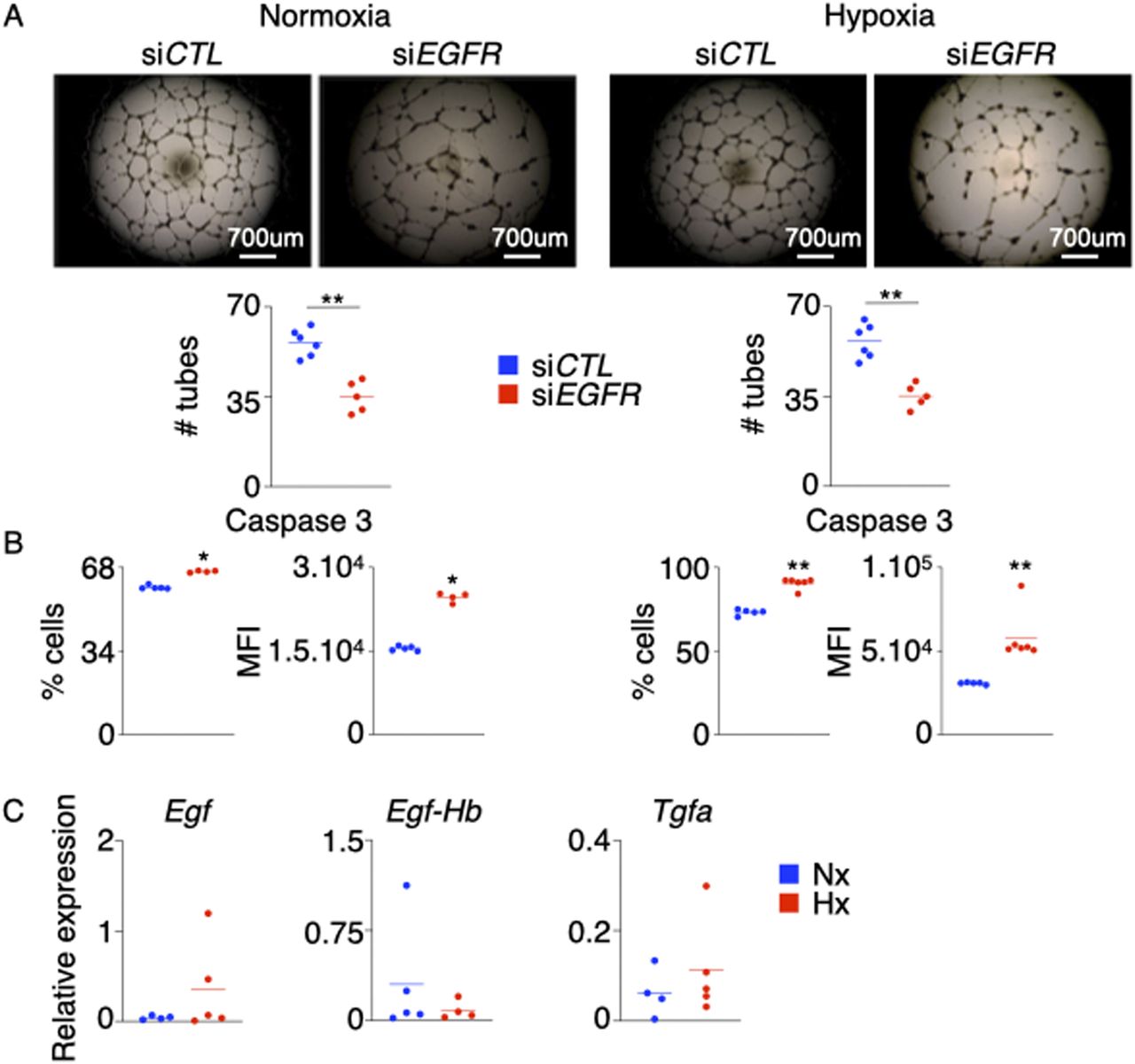
- Figure S3. EGFR silencing in HPAECs decreases their angiogenic ability and increases cell death.
HPAECs were transfected with either siEGFR or siCTL and were exposed to normoxia (left panel) or hypoxia (right panel) for 24 h. (A, B) Angiogenesis was assessed by tube formation assay (A), and apoptosis was measured by flow cytometry (B). (C) Egf, Egf-Hb, and Tgfa were measured in the lungs of hypoxic mice. Data are shown as mean. **P < 0.01.
- Figure S4. AREG and Egfr deficiencies increase pro-inflammatory cytokine expression and modulate pro-fibrotic gene expression in pulmonary arterial endothelial cells.
(A, B) Human pulmonary arterial endothelial cells were transfected with siAREG for 72 h and placed in hypoxia or normoxia for 24 h. (A) The supernatants were collected at 72 h post treatment, and IL-1β, IL6, and TNF-α levels were measured by ELISA. (B) TGFB and SMAD1, 5, and 9 expression was assessed by RT-qPCR. (C) Cdh5+/+ Egfrfl/fl and Cdh5cre/+ Egfrfl/fl mice were placed in either normoxic or hypoxic conditions for 21 d, and lungs were harvested. Tgfb and Smad1, 5, and 9 gene expression was quantified by RT-qPCR. Data are shown as mean. *P < 0.05, **P < 0.01, ****P < 0.001.
- Figure 3. The loss of AREG and Amphiregulin receptor epidermal growth factor receptor (EGFR) in ECs increases their inflammatory phenotype.
(A) Pulmonary arterial endothelial cells were transfected with either scrambled siRNA (siCTL) or siRNA against AREG (siAREG) and placed in normoxic or hypoxic conditions. IFNB, IL1B, IL6, TNFA, and ARE expression was assessed by qRT-PCR. (B) Cdh5+/+ Egfrfl/fl and Cdh5cre/+ Egfrfl/fl mice were placed in normoxia or hypoxia for 21 d, and lungs were harvested. Ifnb, Il1b, Il6, and Tnfa expression was evaluated in whole lungs by qRT-PCR. (A, B) n = 5 samples (A)/mice (B) per condition. Data are shown as mean. *P < 0.05, **P < 0.01, ****P < 0.001.
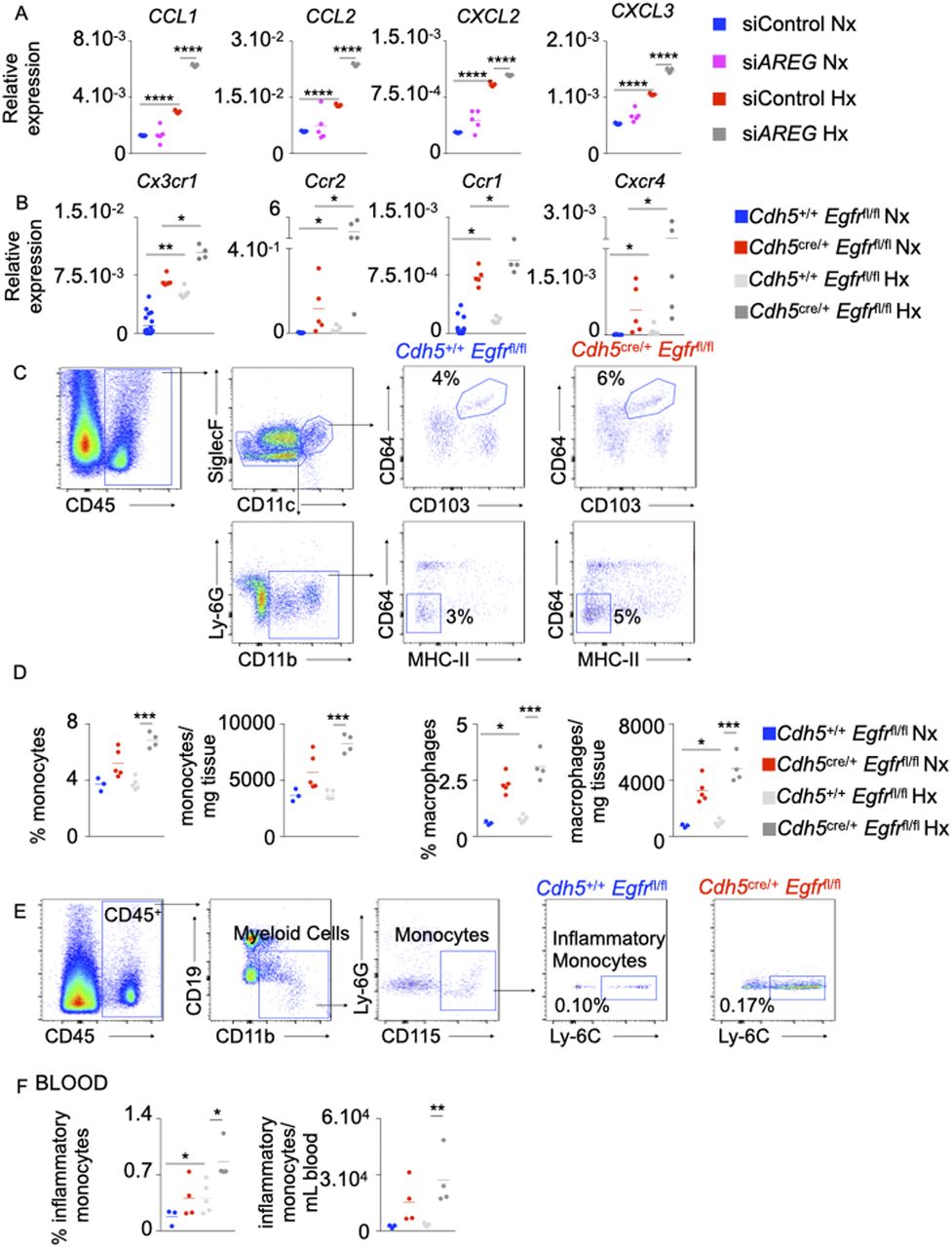
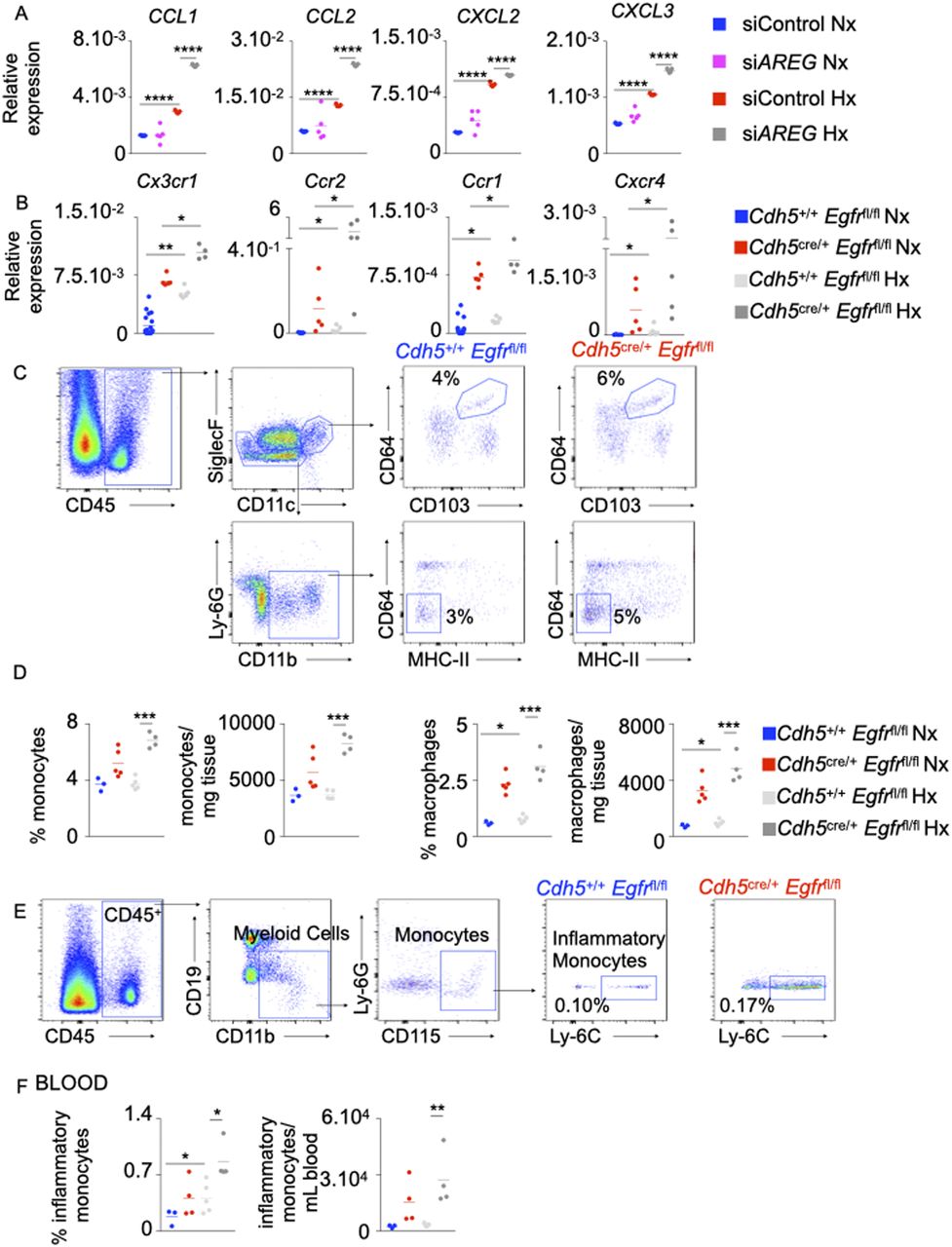
- Figure 4. The loss of AREG and Egfr in pulmonary arterial endothelial cells recruits inflammatory myeloid cells into the lungs in hypoxic mice.
(A) Human pulmonary arterial endothelial cells were transfected with either scrambled siRNA (siCTL) or siRNA against AREG (siAREG) and placed in normoxic or hypoxic conditions. CCL1, CCL2, CXCL2, and CXCL3 expression was measured by qRT-PCR. (B) Cdh5+/+ Egfrfl/fl and Cdh5cre/+ Egfrfl/fl mice were placed in normoxic or hypoxic conditions for 21 d, and lungs were harvested. Cx3cr1, Ccr2, Ccr1, and Cxcr4 expression was assessed in whole lungs by qRT-PCR. (C, D, E, F) Number and frequency of alveolar macrophages (CD45+, CD11c+, CD103+, and CD64+) and monocytes (CD45+, Siglec F−, CD11b+, MHC-II−, and CD64−) were assessed in the lungs (C, D) and blood (E, F) of hypoxic Cdh5+/+ Egfrfl/fl and Cdh5cre/+ Egfrfl/fl mice by flow cytometry. (A, B, C, D, E, F) n = 5 replicates (A) and 5 mice (B, C, D, E, F) per condition. Data are shown as mean. *P < 0.05, **P < 0.01, ***P < 0.005, ****P < 0.001.
- Figure S5. Absence of Egfr in murine lung ECs increases the number of pro-inflammatory macrophages.
(A, B) Lung sections of mice conditionally lacking Egfr in ECs were stained for CD68 (green), iNOS (white, A) and Arg1 (red, B). (A, B) The numbers of iNOS+ (A) and Arg1+ (B) macrophages were quantified by confocal imaging. (C, D, E) Human pulmonary arterial endothelial cells (PAECs) were transfected with either scrambled siRNA (siCTL) and siRNA against AREG (siAREG) and placed in a transwell chamber. They were then cultured in hypoxic conditions with or without leukocytes for 24 h. (C) AREG expression was assessed in leukocytes and HPAECs by qPCR. (D) Apoptosis of normoxic and hypoxic HPAECs was quantified by flow cytometry and shown as fold change compared with the level of apoptosis in siCTL PAECs. (E) HPAECs were plated on Matrigel, and tube formation was measured. (F) Human PAECs were treated with increasing concentrations (10–100 ng/ml) of recombinant amphiregulin or vehicle and placed under normoxic conditions. PAECs apoptosis was assessed by measuring caspase 3+ cells and caspase 3 MFI by flow cytometry. Isotype control was used to determine caspase 3 positivity. n = 5 replicates per condition. Data are shown as mean. *P < 0.05, **P < 0.01, ***P < 0.005, ****P < 0.001.
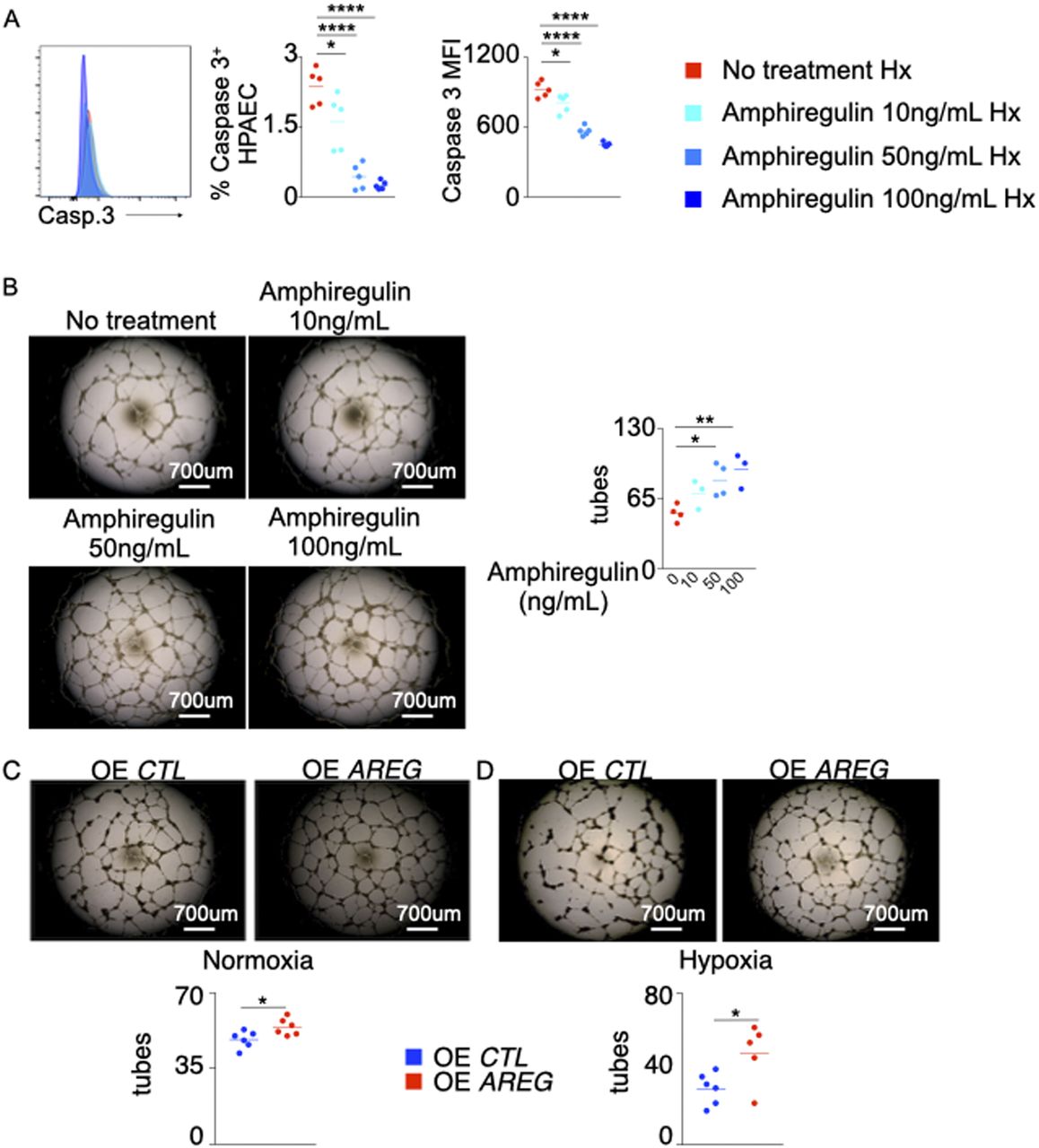
- Figure 5. Amphiregulin treatment decreases pulmonary arterial endothelial cell (PAEC) apoptosis and increases tube formation.
PAECs were treated with increasing concentrations (10–100 ng/ml) of recombinant Amphiregulin or vehicle and placed under hypoxic conditions. (A) PAEC apoptosis was assessed by measuring caspase 3+ cells and caspase 3 mean fluorescence intensity (MFI) by flow cytometry. (B) The cells were plated on Matrigel after the treatment, and tube formation was assessed. (C, D) PAECs were transfected with either an empty plasmid (OE CTL) or a plasmid encoding AREG (OE AREG) and placed in either normoxic (C) or hypoxic (D) conditions. The tube formation ability of the transfected PAECs was assessed. n = 5 replicates per condition. Data are shown as mean. *P < 0.05, **P < 0.01, ****P < 0.001.
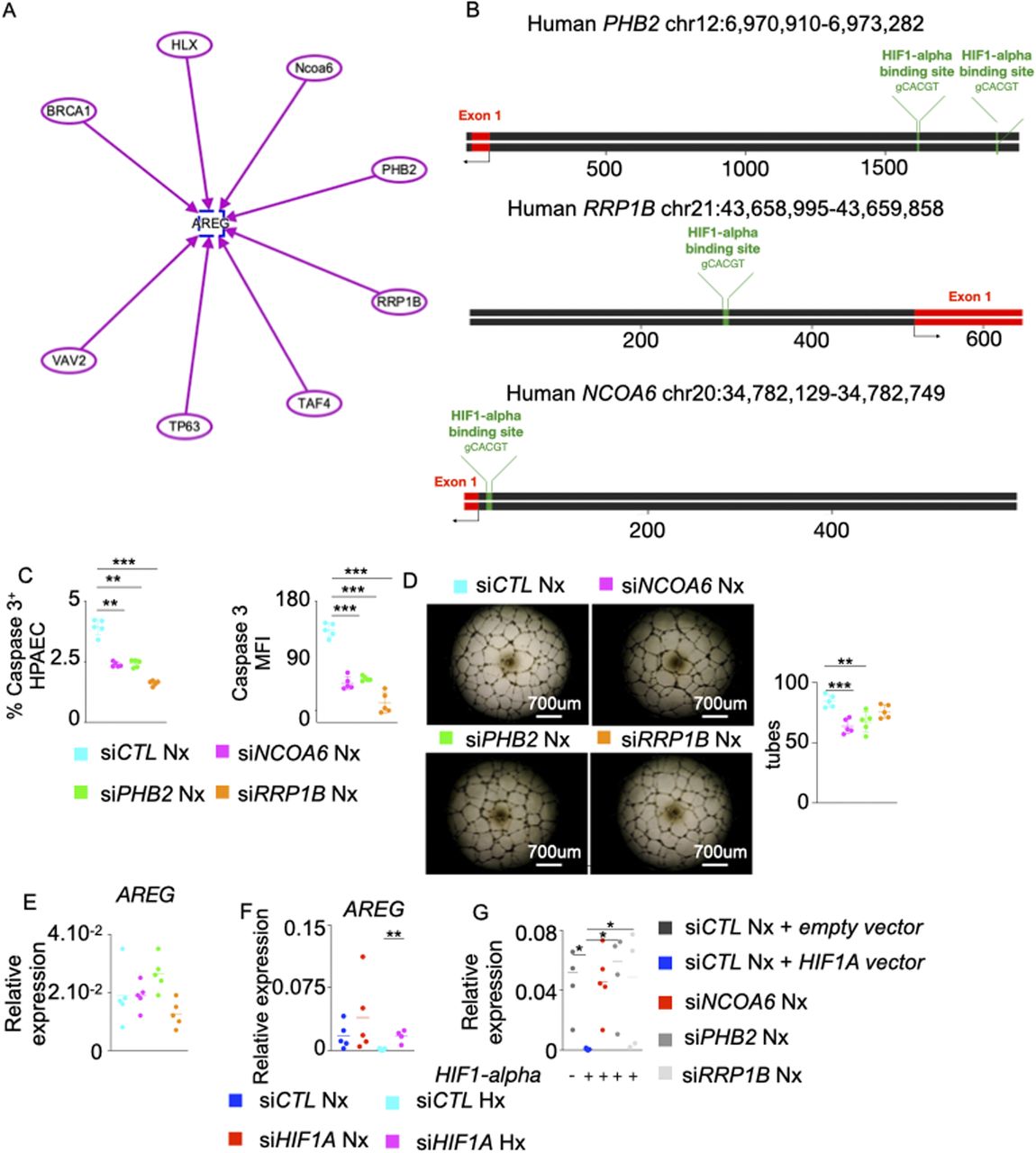
- Figure S6. AREG suppression by NCOA6, PHB2 and RRP1B is HIF-1⍺-mediated.
,(A) Schematic representing AREG and its upstream genes including BRCA1, HLX, NCOA6, PHB2, RRP1B, TAF4, TP63, and VAV2 was generated using the Ingenuity Pathway Analysis Software. Each arrow represents the activation of AREG by each gene. (B) Schematic depicting HIF-1⍺–binding sites in PHB2, RRP1B, and NCOA6 gene promoter regions. This schematic was designed using UCSC Genome Browser website (https://genome.ucsc.edu) and Snapgene software (https://www.snapgene.com). (C, D, E) Pulmonary arterial endothelial cells (PAECs) were transfected with scrambled siRNA (siCTL) or siRNA against NCOA6 (siNCOA6), PHB2 (siPHB2) or RRP1B (siRRP1B) and placed in normoxia for 24 h. (C) Apoptotic PAECs were quantified by measuring caspase 3+ cells and caspase 3 MFI by flow cytometry. (D) PAECs were plated on Matrigel, and tube formation was assessed. (E) AREG expression was assessed by qPCR. (F) Human PAECs were transfected with either scrambled siRNA (siCTL), or siRNA against HIF1A and placed in normoxic or hypoxic conditions for 24 h. AREG expression was quantified by qPCR. (G) Human PAECs were transfected with a lentivirus overexpressing HIF1-A for 48 h. The cells were transfected with siRNA against NCOA6, PHB2, or RRP1B and cultured in normoxic conditions for 48 h. AREG expression was assessed by qPCR. n = 5 replicates per condition. Data are shown as mean. *P < 0.05, **P < 0.01, ***P < 0.005.
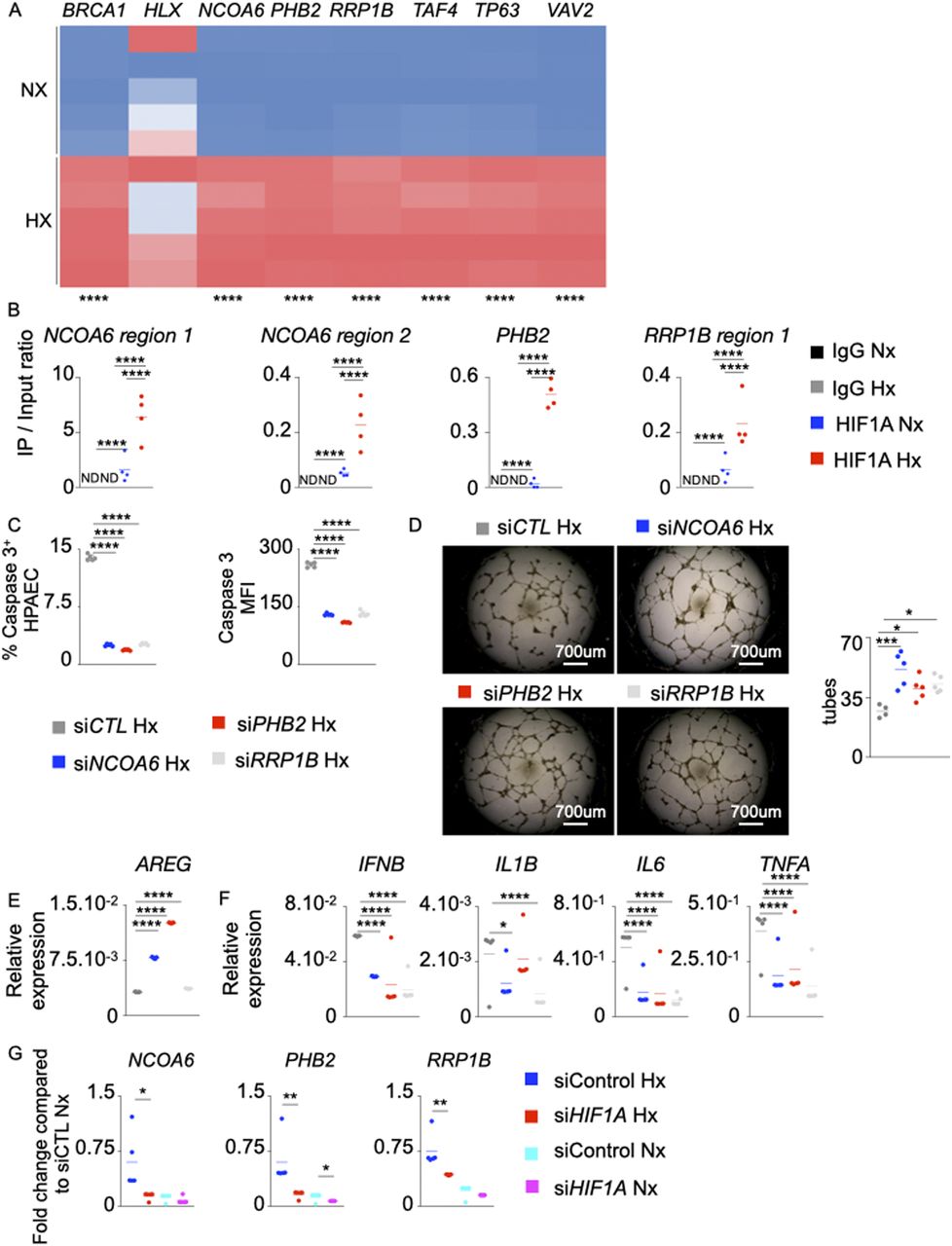
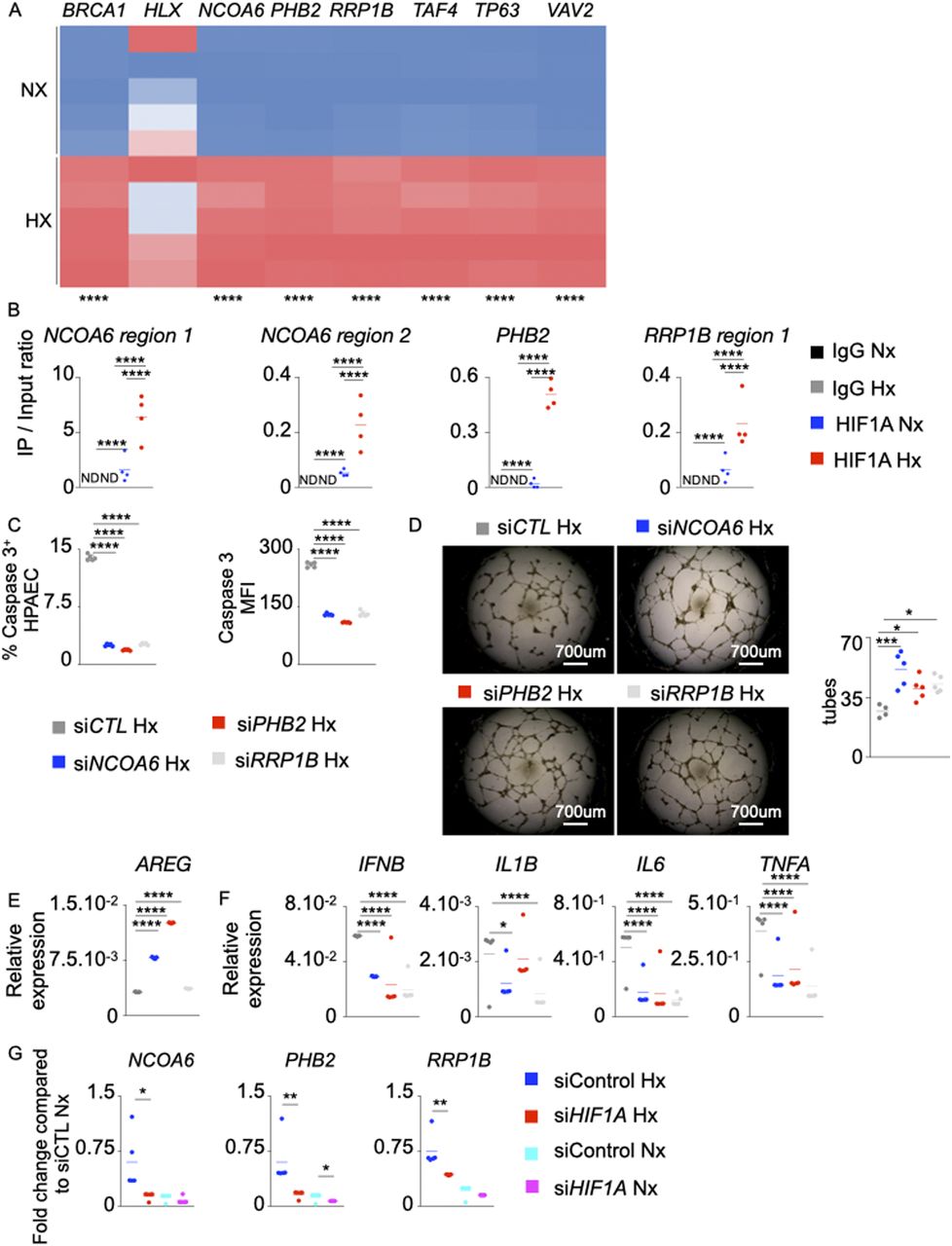
- Figure 6. Hypoxia inducible factor-1⍺ (HIF-1⍺) negatively regulates AREG expression in pulmonary arterial endothelial cells (PAECs) under hypoxic conditions.
(A) Heat map showing BRCA1, HLX, NCOA6, PHB2, RRP1B, TAF4, TP63, and VAV2 expression assessed by qRT-PCR in normoxic and hypoxic PAECs. (B) The binding of HIF-1⍺ to the NCOA6, PHB2, and RRP1B promoter regions in PAECs was assessed by ChIP qPCR. (C, D, E, F, G) PAECs were transfected with scrambled siRNA (siCTL) or siRNA against NCOA6 (siNCOA6), PHB2 (siPHB2), or RRP1B (siRRP1B) and placed in hypoxia for 24 h. (C) Apoptotic PAECs were quantified by measuring caspase 3+ cells and caspase 3 MFI by flow cytometry. (D) PAECs were plated on Matrigel, and tube formation was assessed. (E, F) AREG (E), IFNB, IL1B, IL6, and TNFA (F) expression was assessed by qRT-PCR. (G) PAECs were transfected with either scrambled siRNA (siCTL) or siRNA against HIF1A (siHIF1A) and placed in hypoxia or normoxia for 24 h. NCOA6, PHB2, and RRP1B expression was quantified by qRT-PCR. n = 5 replicates per condition. Data are shown as mean. *P < 0.05, **P < 0.01, ***P < 0.005, ****P < 0.001.
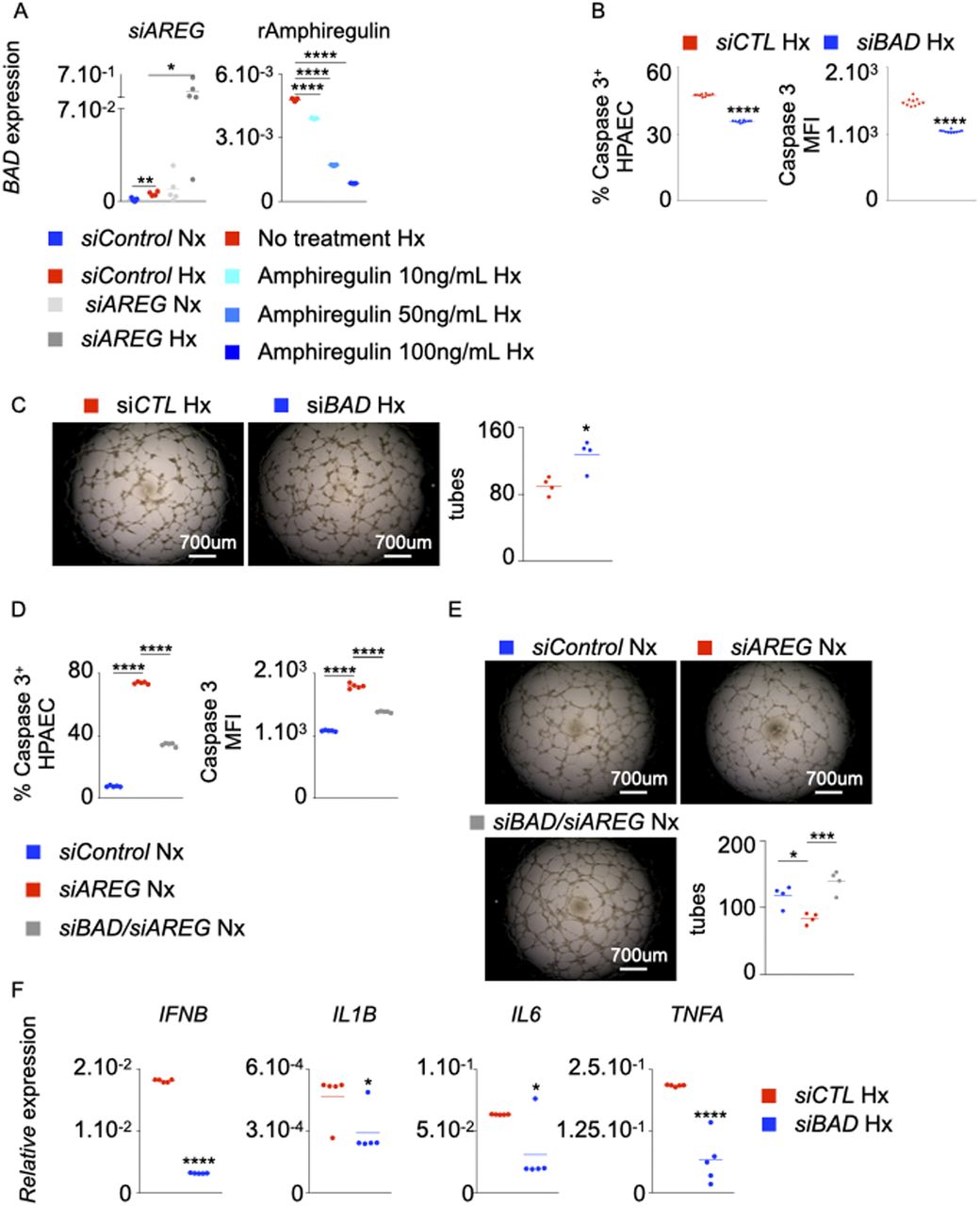
- Figure 7. BAD is essential for exaggerated inflammation, enhanced apoptosis, and suppressed tube formation ability of ECs in the absence of AREG.
(A) BAD expression in pulmonary arterial endothelial cells (PAECs) was quantified after AREG silencing (left panel) and recombinant Amphiregulin treatment (right panel). (B, C, F) PAECs were transfected with either scrambled siRNA (siCTL) or siRNA against BAD (siBAD) and placed in hypoxia for 24 h. (B, C) PAECs apoptosis was assessed by measuring caspase 3+ and caspase 3 MFI cells by flow cytometry (B), and tube formation ability was determined by a Matrigel assay (C). (D, E) PAECs were transfected with either scrambled siRNA (siCTL), siRNA against AREG (siAREG) or siRNA against both AREG and BAD (siBAD/AREG) and placed in normoxic conditions for 24 h. (D, E) Apoptosis (D) and tube formation (E) were examined. (F) IFNB, IL1B, IL6, and TNFA expression was assessed by qRT-PCR. n = 5 replicates per condition. Data are shown as mean. *P < 0.05, ***P < 0.005, ****P < 0.001.
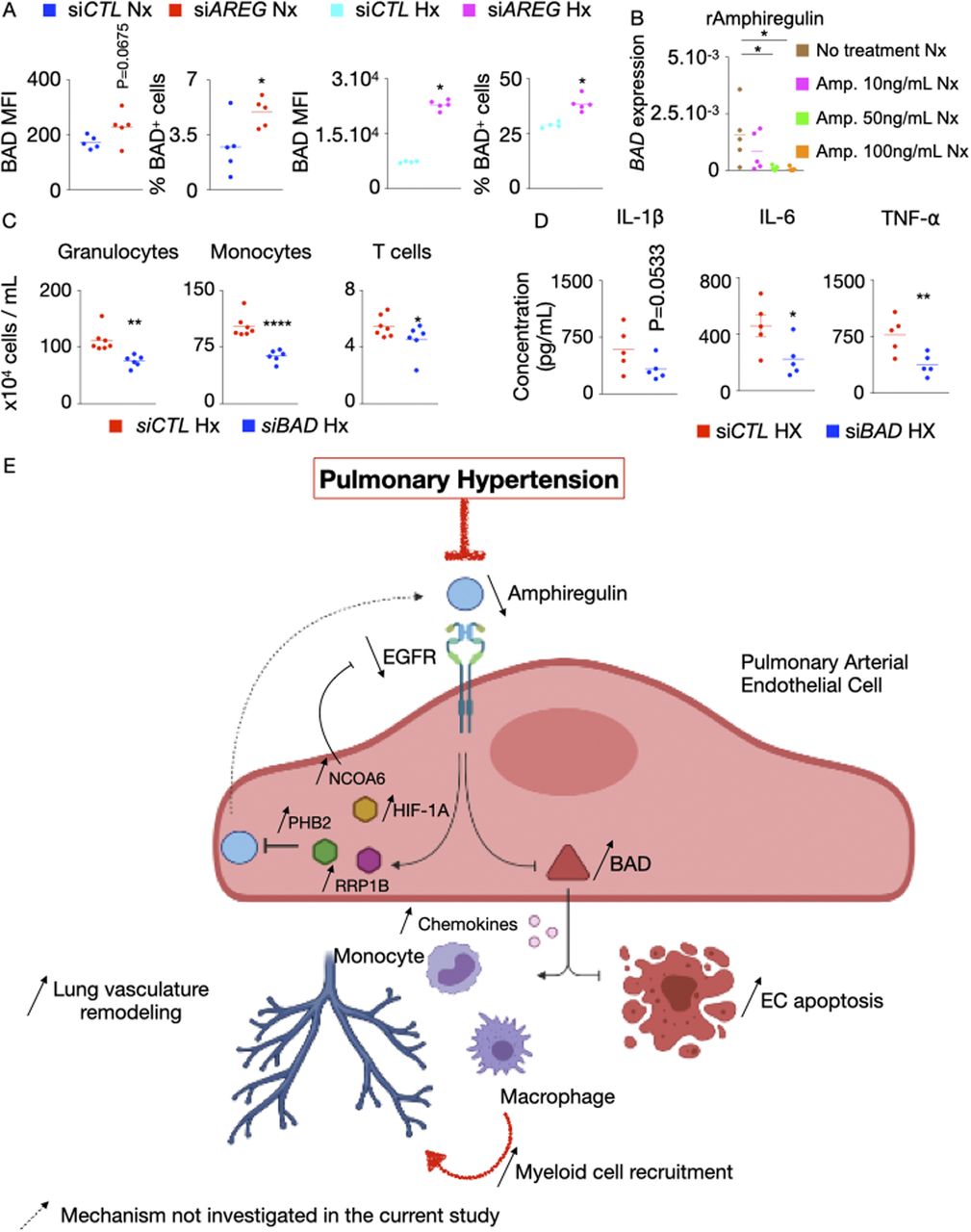
- Figure S7. BAD increases inflammation and leukocyte recruitment in hypoxic HPAECs.
(A) BAD expression and the frequency of BAD+ cells were determined by flow cytometry after AREG silencing in normoxic and hypoxic pulmonary arterial endothelial cells (PAECs). (B) PAECs were treated with increasing concentrations (10–100 ng/ml) of recombinant amphiregulin or vehicle and placed under normoxic conditions. BAD expression was measured by RT-qPCR. (C, D) HPAECs were co-cultured in a transwell with leukocytes and then treated with either control or BAD siRNA. (C) Granulocytes, monocytes, and T cells were enumerated by flow cytometry. (D) Cytokine concentrations were assessed by ELISA. (E) Mechanisms of increased PAEC apoptosis and exaggerated inflammation in the absence of AREG and epidermal growth factor receptor (EGFR) in pulmonary hypertension (PH). Our data support a model whereby decreased amphiregulin and EGFR expression in PAECs promote PH. Specifically, in the steady state, amphiregulin binds to the EGFR, which decreases the expression of BCL2-associated agonist of Cell Death (BAD), resulting in PAEC survival and suppressed inflammation. In PH, HIF-1⍺ binds to the promoters of NCOA6, PHB2, and RRP1B and increases their expression. These genes down-regulate AREG, resulting in augmented BCL2 expression. This pro-apoptotic gene, in turn, incites apoptosis and chemokine production. Elevated levels of the chemokines recruit inflammatory myeloid cells in lung vasculature. Mechanisms that were not investigated in the present study are labeled with a dotted arrow. The cartoon was designed with the online Biorender software (https://biorender.com). n = 5 replicates per condition. Data are shown as mean. *P < 0.05, **P < 0.01.












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}

In this Issue
Subjects
Related Articles
Cited By...
- Identification of key genes and biological pathways in chronic obstructive pulmonary disease using bioinformatics and next generation sequencing data analysis
- Transcriptional profiling of skin cancer NK cells reveals the elevated glucocorticoid signaling switches their anti-tumor characteristics to a homeostatic feature